The question of how to describe and categorize addiction has been the subject of several of my recent posts. Some people scratch their heads about why I care so much about whether we think of it as a disease. Bill White summarized the stakes well here:
If AOD problems could be solved by physically unraveling the person-drug relationship, only physicians and nurses trained in the mechanics of detoxification would be needed to address these problems. If AOD problems were simply a symptom of untreated psychiatric illness, more psychiatrists, not addiction counselors would be needed. If these problems were only a reflection of grief, trauma, family disturbance, economic distress, or cultural oppression, we would need psychologists, social workers, vocational counselors, and social activists rather than addiction counselors. Historically, other professions conveyed to the addict that other problems were the source of addiction and their resolution was the pathway to recovery. Addiction counseling was built on the failure of this premise.
White, W. (2004). The historical essence of addiction counseling. Counselor, 5(3), 43-48.
Whether we define alcoholism as a sin, a crime, a disease, a social problem, or a product of economic deprivation determines whether this society assigns that problem to the care of the priest, police officer, doctor, addiction counselor, social worker, urban planner, or community activist. The model chosen will determine the fate of untold numbers of alcoholics and addicts and untold numbers of social institutions and professional careers.
The existence of a “treatment industry” and its “ownership” of the problem of addiction should not be taken for granted. Sweeping shifts in values and changes in the alignment of major social institutions might pass ownership of this problem to another group.
White, W. L. (1998). Slaying the Dragon: The History of Addiction Treatment and Recovery in America, page 338
I’ll acknowledge that hustles like patient brokering, cash MAT clinics, drug screen scams, and over-priced residential with little continuing care make it difficult to root for the survival of the “treatment industry” but White’s words capture the risks of transferring responsibility to other groups.
What’s made addiction counseling unique has been the emphasis on recovery as the endpoint. More specifically, a model of recovery that results in people with addiction becoming “better than well.”
An essential step in transferring responsibility from one group to another is redefining the problem.
Some efforts to define addiction as something other than a disease argue that it’s not a disease but, more often, arguments against the disease model are more about achieving particular goals (protecting liberties, assigning personal responsibility, advancing particular drug policy goals, advancing social justice, emphasizing particular interventions, stigma reduction, etc.) rather than questioning whether it’s actually a disease.
Recently, the American Journal of Public Health published an article titled The Harms of Constructing Addiction as a Chronic, Relapsing Brain Disease. I appreciated the clarity of its arguments.
The article opens with the following paragraph:
As an international network of historians and social scientists who study approaches to the management of drugs across time and place, we have noticed the effort to redefine addiction as a chronic, relapsing brain disease (CRBD). The CRBD model is promoted as a route to destigmatize addiction and to empower individuals to access treatment that works within that model’s terms.1 CRBD usefully recognizes that brain-based neural adaptations place individual brains in chronic states of readiness to relapse. But brains are housed inside of people. Substance use is biological, social, and political; our concepts and approaches to complex questions surrounding substance use must be, too.2,3 By overlooking the sociopolitical dynamics and inequalities bound up with substance use, the CRBD model can paradoxically further marginalize people who use drugs by positing them as neurobiologically incapable of agency or choice. We are concerned that the CRBD model paints drug users as individuals whose exclusion from social, economic, and political participation is justified by their biological flaws and damaged brains.
Note that the authors respond to an argument for what the disease model can accomplish — it “is promoted as a route to destigmatize addiction and to empower individuals to access treatment” — rather than to the argument that it is properly classified as a disease.
All illnesses occur within people and have biological, social, and political contexts. The past couple of years have reinforced that those contexts have important implications, even with something as seemingly straightforward as a respiratory illness caused by a virus. That COVID is associated with social, economic, and political disruption, conflict, and suffering shouldn’t and wouldn’t lead us to questions about whether COVID is properly framed as a disease.
Choosing between the CRBD model and addressing the sociopolitical dynamics and inequalities seems like a false choice. Why does it have to be either/or? Cant it, shouldn’t it, be both/and?
No responsible advocate of the chronic relapsing brain disease (CRBD) model would argue that people with addiction are incapable of agency or choice. Addiction is a disorder involving choice, but it is typically characterized as impaired choice or intermittent loss of choice, rather than a complete or consistent loss of choice. One might compare this to serious mental illness with intermittent fluctuations in impairment. These fluctuations in impairment may range from no impairment to severe impairment, depending on the individual and the current state of their illness.
It’s also important to note the authors’ switch from discussing the CRBD model in the context of people with addiction to people who use substances. The CRBD model should never be applied to people without addiction.
The article proceeds with a brief examination and critique of the CRBD model. The authors note that advocates of the CRBD model voiced hope that the model would produce a sharp break from the moral models that had dominated responses to addiction.
The supposedly new CRBD model recycles disease concepts that have mixed medical and moral concerns since the 18th century.9 Disease models have been used to support a range of policy approaches from strict prohibition, to compulsory treatment or “civil commitment,” to medical maintenance, to incarceration. In them, addiction has been both criminalized and medicalized; addicts were labeled as sick individuals yet also punished for bad behavior as deviants….
Despite the hopes placed on the new CRBD model, this heritage has not been erased by redefining addiction as a chronic disease located in the brain.11 On the contrary, the brutal social inequalities of US responses to drug-related harms have persisted or even worsened.
Note that this is not actually criticism of the CRBD. Rather, it’s criticism of the fact that the CRBD has not delivered the change in policy and attitudes that many people hoped for.
Framing Addiction as a Chronic, Relapsing Brain Disease
The article continues with the suggestion that the CRBD may have accelerated these harms in ways that include criminalization, incarceration, and a molecular orientation that opened the door for the opioid crisis with the false belief that Oxycontin’s extended-release formulation might make it safer.
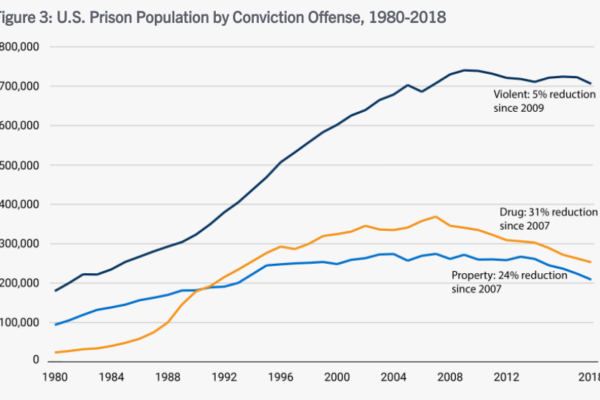
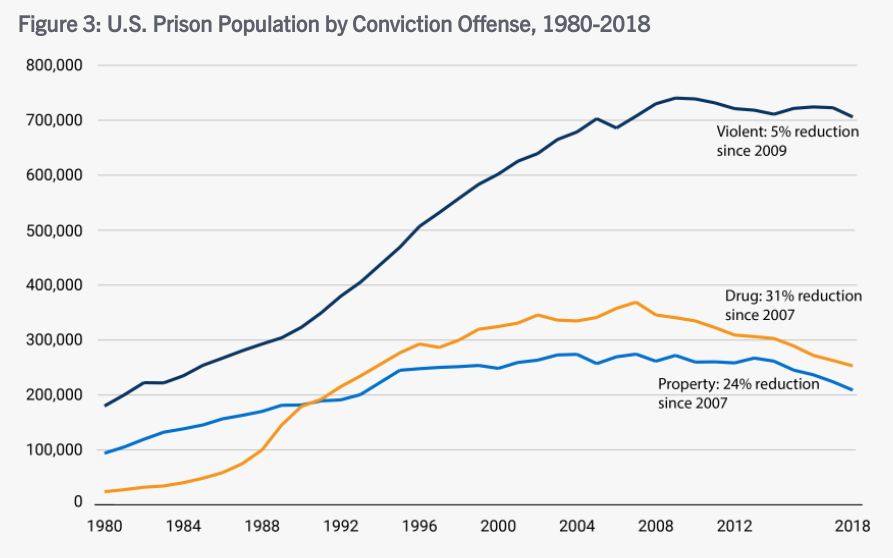
I’m not a believer that the CRBD necessarily leads to less stigma and better policy, and I won’t suggest that the CRBD is responsible for any changes in policy. However, the argument that the CRBD model is associated with incarceration is undermined by trends in incarceration for drug crimes. Even if the CRBD model could deliver significant policy and cultural change, that would take time — years, probably many years. The chart below shows a leveling off and eventual decline of people incarcerated for drug crimes during the period discussed. It’s still too many people incarcerated and those people are disproportionately African American but, if we want to assert an association between the CRBD and incarceration rates, the association would be a downward trend in drug crime incarcerations.
-

A liver cure containing 90% alcohol. -
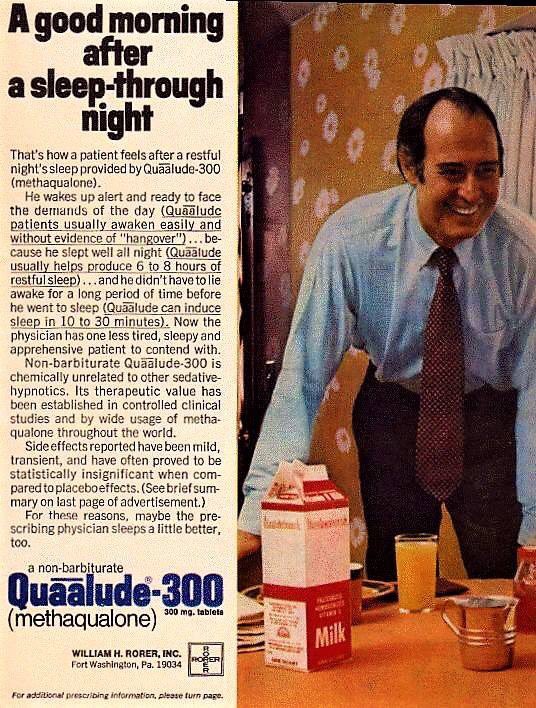
“mild… statistically insignificant side effects”
The Oxycontin argument would be a lot stronger if there wasn’t a long history of pharmaceutical advertising that misrepresented the safety profile of medications, often misrepresenting science to obscure the risks.
So… the criticism is not about the scientific or medical truth of the model, rather it’s about insufficient political and social progress.
This section ends with a strong point:
Expanding access to addiction medications without inclusive social policies and harm reduction has not been enough to prevent or stem America’s opioid crisis.
Calling something a brain disease does not and should not narrow our attention to pills and procedures. Behavioral, psychological, and social interventions ought to be particularly important with a brain disease, particularly since a brain disease is likely to affect those domains and those domains are largely experienced in the brain.
Alternate Frame: Harm Reduction and Social Justice
The authors offer harm reduction and social justice as an alternative frame:
There are other ways of framing and responding to substance use. The most promising of these is harm reduction, a 50-year-old social movement mounted against repressive drug policies. Rather than centering on the brain and embracing abstinence as a goal, harm reduction prioritizes the health and social inclusion of people who use drugs.
Note that the authors are not really speaking to causes or treatments and there’s no reason the recognition of a condition as a disease should omit social inclusion. For example, serious mental illnesses are recognized as diseases and social inclusion should be considered an essential element of effective treatment and policy.
So, what is the concern?
Consumers resist the coercive and often punitive ways in which medications for addiction have been deployed. Harm reduction links the biological to the social without prioritizing one over the other.
So, a concern is coercion. Calling something a brain disease does not necessitate coercion (think Parkinson’s), but it can open the door. In the medical world, that door might be opened through the legal designation of a guardian. With mental illness, involuntary treatment may be sought for patients that pose a risk to themselves or others. In the cases of guardianship and court-ordered treatment for a mental health crisis, there are processes designed to protect the rights of the individual, including time limitations on any court order resulting from the process.
In the case of addiction, involvement with the criminal justice system often leads to coerced treatment. And, there has been far too little systemic ambivalence about individual rights when it comes to coerced treatment (and incarceration) for addiction. Importantly, there’s also been too little concern about systemic injustices, like the disproportionate numbers of African Americans charged and convicted of drug crimes.
Addiction is also unusual among diseases in an important way. As Keith Humphreys pointed out, “To use a term from economics, addictions have high negative externalities that most medical disorders simply do not, and that changes how perfectly decent and reasonable people respond to them.”
To illuminate those high negative externalities, Humphreys poses the following questions:
If you had a financial manager who would have access to all your accounts and personal information, would you consider that person developing a heroin addiction of any more consequence than him/her developing type 2 diabetes? If you were enrolling your child in a preschool, would you react in the same way if informed that the teacher was prone to methamphetamine binges as you would to learning that the teacher was prone to asthma attacks? If asked by a non-expert from outside our field, how would you explain why millions of people have chosen to attend self-help groups and treatment programs focused on recovering from having had an ‘‘alcoholic’’ parent, but there is no demand for recovery programs focused on adult children of hypertensive patients?
Acknowledging that there has been insufficient concern for individual rights, I suppose at least 4 considerations are important regarding coerced treatment.
- Do the circumstances merit limiting the liberties of the person (through court supervision, incarceration, or coerced treatment)? Is this a circumstance where others were harmed or at serious risk of harm? If we removed the substance from the situation, would this still be a matter for the criminal justice (or child protection) system?
- Treatment for what? What is the person’s substance use problem and is the treatment appropriate for that problem? Are we talking about someone with a mild, moderate, or severe problem? Are we talking about someone with a pattern of impaired control?
- Coerced treatment is often an alternative to incarceration. This is a good thing. However, we should be mindful that this option doesn’t lower the bar for limiting the rights of a person.
- What systemic factors are likely to influence who ends up in this system and how their case is handled? Are we acknowledging and addressing those? If forces external to this system are a problem, how can that be mitigated within this system?
I’m ambivalent about the development of processes for addiction that would mirror the mental health processes. Having worked in both systems, I know it would require a lot of work to protect the rights of people with addiction and an enormous amount of work to develop systems of care that can meet the need effectively.
As for the role of the CRBD model in this area, I do see the risk and I do sometimes hear the CRBD model deployed to defend coerced treatment. At the same time, the period of time the authors point to has been characterized by efforts to reduce incarceration and offer treatment as an alternative — on the grounds that addiction is an illness.
I think the CRBD model offers a valuable test for public policy — parity. Would we, should we, treat a cardiac or diabetes patient this way? The high negative externalities identified by Humpreys do present a challenge for parity tests using other chronic diseases, but he offers another frame. He’s talking about it in the context of public education, but it’s relevant for thinking about policy as well.
A better analogy than asthma, type II diabetes, and hypertension we could employ for addiction might be to liken it to chronic infectious illnesses (eg, HIV/AIDS). We accept that for infectious illnesses, some fear of people who have the disease is rational; indeed health professionals exhort people to engage in behavior designed to protect themselves from infected individuals (eg, insisting that a sexual partner with a sexually transmitted disease wear a condom, not personally cleaning the body of someone who died from Ebola). Further, we accept that there is a legitimate role for law enforcement— Typhoid Mary was prevented from continuing to infect people by police (Marinelli et al., 2013), not doctors. Analogizing addictions to infectious diseases has all the virtues of analogizing it to diseases with low externalities (eg, asthma) and also has the unique advantage of better matching the public’s experience of the disorder (and it is them and not ourselves whom we need to persuade).
Of course, this imagery will evoke strong negative reactions from many, but it also provides the potential to narrow the focus for coercive interventions to those where there is actual harm or serious risk to others.
Uneven Progress: Harm Reduction in Europe
Next, the authors provide a little background on harm reduction in Europe that they summarize as follows:
Harm reduction initiatives across Europe and the United Kingdom were introduced as part of publicly funded institutions that often coexist with repressive drug policy systems—something shown with unusual starkness in the French example. The UK example indicates how harm reduction measures do not always center on social justice for people who use drugs but are instead introduced to protect the majority population. The Norwegian example points toward how restrictive access to harm reduction services can facilitate paternalism and reduce agency of people who use drugs.
Conclusion: Human Rights as an Expanded Harm Reduction Frame
…The human rights frame counters some of the CRBD model’s limitations, including the centering on brain disease pathology and insistence on judging each individual as either a patient or a criminal.
People who use drugs are themselves developing community-based harm reduction approaches that resist both criminalization and medicalization on the ground that both have been used to control drug users. Harm reduction critiques hierarchical forms of clinical and neuroscientific expertise and instead supports people who use drugs in recognizing their expertise in managing their own practices and bodies, supporting their agency, and widening their options. Abstinence can be considered part of this approach, but only if chosen by people who use drugs themselves.31 When abstinence is imposed by external forces (medical practitioners, family, law enforcement, or other stakeholders), abstinence itself becomes a risk for overdose death.
This illuminates another objection, that the disease label situates the person with addiction as a patient. (As opposed to a criminal.) It’s also important to note that the authors switched from addiction to “people who use drugs.” This switch is important because using drugs isn’t a disease but may be a symptom of the disease of addiction, just as coughing isn’t tuberculosis. To be sure, most people who use drugs do not have the disease of addiction. Differentiating between people with addiction and other people who use drugs is critically important in many ways, but particularly important when discussing the disease model, its conceptual boundaries, and its utility.
The framework of disease is helpful because it helps us draw a boundary to determine who has the disease and who does not, it can help us understand some of the processes involved and their consequences, it can help us identify treatments, and help us identify treatments, behaviors, and interventions that are contraindicated.
The authors seem to be very focused on protecting the right to choose to use drugs. For the minority of users with addiction, a critical element to understand is impaired control, meaning that drug use is not always freely chosen. (One might even say that, at times, the illness coerces the sufferer to use drugs. This is part of what’s so excruciating for people with addiction and their loved ones.) This is one of the reasons that, for this most severe form of drug problems affecting a minority of users, abstinence is indicated.
People with bipolar or schizophrenia have the right to refuse treatment in most circumstances. However, when their illness results in high negative externalities, they may be coerced into treatment via a process that includes several safeguards to protect their liberties.
So… this critique never seems to make a case that addiction is not a disease. Rather, it argues that the CRBD model has not delivered the change some people promised and they proposed a model centered on the social and political change. I don’t see where an emphasis on social justice requires the abandonment of the disease model. In fact, where high negative externalities are present, the disease model becomes a mitigating consideration, resulting in more just social responses.
I believe it’s true that addiction is a disease and the authors never really made an argument that it isn’t. Should that truth be sacrificed or obscured in pursuit of justice? I don’t think it’s a good idea. It’s the kind of thing that contributes to the current epistemic crisis and it isn’t necessary. Any model can be harmful if it’s misused or implemented in a reductive way that results in the neglect of important considerations. The CRBD is no different.