Who are you?
My name is Sam Price, I am the President/CEO for the Ten16 Recovery Network.
Tell me a little bit about Ten16 and your role there.

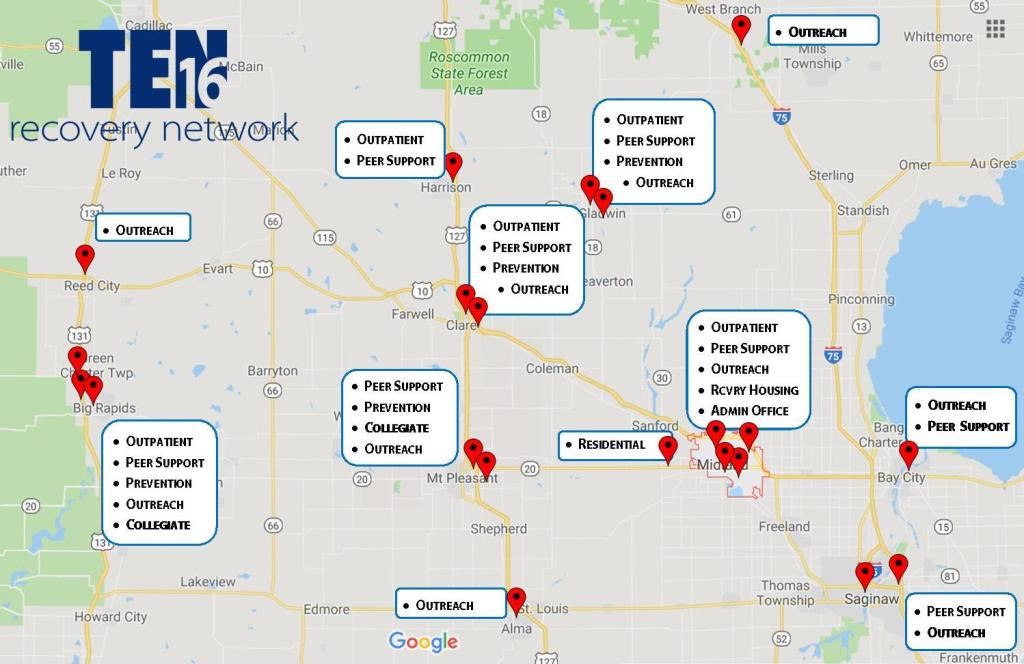
Alright, Ten16 is celebrating its 40th anniversary this year. I have been here since 2003, so about 17 of that has been on my watch. It started out as a halfway house by the local churches, way back in the day, and that migrated into residential treatment, and then we got into outpatient, and then we got into prevention and then we got into expansion. We started in Midland, Michigan. We are now in 10 different counties; providing outreach in emergency departments, we have residential, recovery housing, prevention, outpatient, drop-in centers, collegiate recovery on three campuses, prevention in four, five communities. So we try and have the full continuum, both vertically and horizontally, to work with folks.
How would you describe the communities you’re working in?
It’s a mixture of mostly rural. Midland is probably more of a suburban community. We started to work in Saginaw, which is more urban. So, it’s kind of a broad mixture, but I’d say mostly tilting towards suburban and rural.
Tell us about your professional experience in addiction and recovery, did you have any SUD experience prior to Ten16?
No, I didn’t. When I was selected to come to Ten16, my wife and I lived in Charlotte, Michigan. She was a teacher for the hearing impaired in Lansing, and I worked at a juvenile justice facility called Starr Commonwealth based in Albion, Michigan. Starr had about 200 residential beds for children that were in the juvenile justice system and had sites really across Michigan, in Ohio, with other community-based programs as well as other residential programs. I’ve always been in the helping field in one fashion or another but hadn’t been in SUD specifically. Midland was our hometown, and we wanted to get home. My wife’s mother was sick at the time. The opportunity came up to come to Midland at Ten16 and they invited me to work there, but it was really my first foray into SUD.
What are you most proud of in your professional life?
I saw that question before, and it really made me think…
I think probably the growth of the organization in these recent years, which has been pretty substantial. I think what has most made me proud is the fact that the staff have this willingness to join me to be bold and pioneer. For example, the thing that’s driving us right now is really kind of two ends of the spectrum in terms of how we view what we’re trying to bring to the community. In the one sense, we know that only 10% of the folks that struggle (with SUD) will walk through our doors or your doors on their own. So, we have intentionally said, “How do we put ourselves in places to get in front of the missing 90%?” And how do we engage them in conversations that may spark the beginning of recovery? That shift has attracted to us a lot of people who want to join us in the pursuit of that real… almost… raw recovery evangelism, if you will. So, in the last five to six years, we have ended up going from one hospital Emergency Department to ten; where we can sit with patients who are in the ED, maybe not even because of their SUD history. Maybe they’re there for a broken arm.
Here’s a great example of who we have a chance to talk with – there’s a time that my wife and I were in the emergency room for our own medical situation as a family. In the curtain right next door to where we were, [because that’s the only privacy that you have in the ED], there was a 72-year-old guy who was in there for some cardiac issues. He was waiting for the cardiologist to come, and the nurse came in to do the health history with him. As she’s talking with them, she finds out that he has been a widower for the last three years. He lives outside of Weidman, which is a town that has a population of maybe 1,000 at best. He’s not living even in the town itself, his kids to live out of the state. And, it’s just he and a cat and a six-pack every night.
Now he’s in the ED for heart issues. That’s what our advocates have an opportunity to do. The nurse can then turn to our staff and say, “Hey, I think you need to talk with this guy.” To us, we think there might be something about the six-pack a night that may be contributing to both his physical heart issues and his spiritual heart issues. We’re able to start that conversation that we never get if we just waited for him to walk through our door it. It’s easy to work with the person who shows up under the influence, or who shows up in the ED med seeking and stuff like that. We have so many rich opportunities to talk with other people who we would never normally be able to talk with and engage them in that change process.
On the flip side, we also know that we have to walk alongside somebody for five years before they can get that remission rate down to a truly sustainable level. How do we change our way of doing business and our way of offering services to folks that would cultivate that? We have totally re-engineered our outpatient practice so that it’s full drop-in. Any time you need to stop in and talk with somebody, you don’t have to have a scheduled appointment. You can stop in. The energy that brings to the staff, because we can have this community approach, has been incredible.
Ten16 is a place to start that journey. They can come to this rich, robust community, which then can introduce them to the natural (recovery) community that exists out beyond our professional walls. So, I think that direction, the energy, and the enthusiasm that the staff has brought to that movement would probably be what I would say is my proudest moment at Ten16.
What keeps you working in addiction and recovery?
It’s funny, people ask me that every now and then. When I was much, much younger, I had an opportunity to experience redemption on a personal level, because I was becoming a person that I didn’t think I was up here [pointing to his head – my self-perceptions weren’t in alignment with my actions]. When I really stepped back and saw where my life was heading, that’s not what I wanted to be. There was a spiritual awakening, if you will, that allowed me to experience this sense of redemption. The richness that that has brought (to my life) since then, is something that I want anyone who is lost and hurt and broken to have an opportunity to find. People that struggle with SUD need folks to help stand in the gap and say, “Hope is here and will be here and we’ll be here as long as you need… until maybe you can experience the same thing that I’ve experienced.”
How has the pandemic affected your work at Ten16?
Well, it certainly has put a cramp on community. We have to be uber-cautious for the safety of the staff and the safety of all the clients. There is a fair amount of concern that comes with that, which has a lot of really unhealthy consequences, particularly for the folks that we work with, because it breeds isolation. Isolation strips away the community that had been holding me (speaking as if a person in early recovery) together, and giving me that encouragement that I’ve been looking for in order to be able to keep moving forward every day.
A lot of that’s been stripped away… Yeah, I (speaking as if a person in early recovery) can get it through a virtual meeting, but that’s not the same as being face-to-face with other folks. So, the loss of that is hard. So, a lot of the coping mechanisms that I had have been stripped away from me, and haven’t been replaced in the same kind of meaningful way, and all new kinds of stressors are kinda coming along for us. So, Ten16 has seen an uptick in relapses. We’ve seen a huge uptick in the hospitals for alcohol-related events. They’ve (the hospital staff) seen a big uptick in methamphetamine and opiate relapses too.
So, as so many others in the press have said, it has a secondary impact when you roll into a pandemic with an (opiate) epidemic. It’s just not a good combination at all. The other thing is that, at the same time that it’s impacting all the folks that we serve, it’s impacting everyone that works here at the same time. It is not like there’s this separation. So, I’m trying to be present for the people who are coming to my care, and I still have to think about my wife and my kids–are they safe? and my extended family and my parents, are they safe? –none of us can escape that. It’s not just impacting the folks that we serve, it impacts all of us. So, it’s hard to turn that noise off, to be present, to help those that are looking to us for care at this time.
What, if any, long-term effects do you anticipate from the pandemic for the field?
It’s hard to know fully, because we’re still so early into it. I’m seriously afraid that it could be another 12 or 18 months that this is going to linger, if we have another wave that comes through. What I don’t know is what that’s going mean to treatment facilities. I’ve already heard that several dozen across the state have already closed, and another several dozen are teetering on the brink of closure.
Because of leaders trying to be safe in the way that they run their programs, there is limited access to treatment beds for those people that need a higher intensity of care. So, access is just going to continue to get crippled, which means getting in for timely service is going to be really, really problematic for folks. There are no easy answers to know how to fix that.
Even when you think of what happens out in the natural 12-step community, and the larger recovery community, even that has been impacted. Can there still be meetings indoors? Even so, you can’t have meetings of more than 10 people. Are there in places in our communities (like churches or community centers) that are even allowing 12-step meetings to be hosted because of some of the risks? So, there are so many ripple effects… I think we’re still just at the tip of the iceberg that we just don’t even know yet.
Again, that’s part of the problem, there’s so much uncertainty and ambiguity that is difficult for people to know how to navigate. There’s no end in sight to that, which gets back into that resilience depletion, right?
Have you seen any benefits or new opportunities in the pandemic?
Certainly the one that everyone turns to is the advent of telehealth, both for treatment services as well as recovery support, peer support opportunities. Again, it’s a blessing and a curse thing. Certainly, it fills in some of that access gap that [with a tool] we never had. Because we are forced to do it has made both parties–both providers and participants–more open to that. We find that, “Hey, this is can be a nice thing for me to be able to have my session, but I don’t have to worry about the headaches of transportation, because I don’t have a driver’s license, or I don’t have money for the bus or something along that line.” So, there are huge wins to that. I can go into rooms and I can find a meeting anywhere across the country. Those are wonderful things. There are limits to those things too, so there’s always the concern that when the pendulum swings or when the policy makes you say, “Oh, look at that.” All of a sudden it becomes a substitution for real community, because we’ve been able to develop this virtual community.
As it continues on, I think it will force us to continue to figure out how we can be more creative–how does it force us out of our boxes? For example, the regulations behind telehealth before were just Neanderthal. No one did it because the regs were so tight. Well, this kind of forced that change, and now that that horse is out of the barn, some of the people that hold the dollars have realized, “Okay, maybe we were a little bit too rigid, too cautious in some of the stipulations that were put into place.” Hopefully, that will allow for more creativity and more freedom, more flexibility to spark innovation.
I think we’re still trying to figure it out and figure out what the rules are, of how you can advance things safely within this… if we have to limit the number of people that are in a room, if we have to wear masks, if we have to be 6 feet apart….there are just so many new factors that we have to sort through, that I don’t think we know fully yet. It forces us to get out of our little cookie-cutter approaches that we’ve been so comfortable with–that has defined how we provide care–so I’m excited to see where it may lead us. All of a sudden we could have opportunities where, yes, we’re here in Midland, but all of a sudden maybe because of telehealth, we’re providing treatment and care and support to people in Ohio, or Wisconsin, or Seattle.
I think [peer support among providers via video conferencing] could be another good silver lining. We have gotten very comfortable doing this kind of stuff and feeling good with it.
We’re just talking about that mid-state meeting… if we could just have an open Zoom meeting for any provider that just wants to talk about the stresses, and the strains, and the struggles of doing virtual care, and all this sort of stuff, why wouldn’t we? Why couldn’t we? Maybe it’s breaking down some of those walls that have held us back.
If you were able to devote yourself to a fantasy project to improve treatment and recovery support, what would it be?
Sam: I think we still haven’t figured out as a system of care of how we go beyond maybe that first year of support. As people grow and mature in their recovery, those recovery needs change–how do we walk alongside them in meaningful, productive, and constructive ways?
We often talk within our organization–how do we help people move from recovery into wellness? As I’m getting some of these early recovery skills down, and I’ve figured out this part… but then there’s the next layer of my relationships or I’m getting my relationship with drugs in that right and healthy and place, but now it’s about, how do I find a career that brings me a feeling of meaning and purpose? Or, how do I get my relationships where that brings me meaning and purpose? How do I keep building upon that, in a way that I have constructed this robust life that we all kind of long for and dream for?
I’ve also seen some of those organizations that have micro-enterprises where they employ their own, and then those employees become the managers of different places, and some of those types of organic businesses or organic opportunities would be so cool to see develop.
Another odd little fantasy that I’ve had every now and then is, “I wonder what it would be like to have an assisted living facility for people in long-term recovery?”
I don’t know why, but [the idea has] always been one of those, “Huh, I wonder… as we age… would that be something?”
I don’t know why, but it’s always intrigued me about that kind of a community, and how would that look differently as we age, when typically medications are being poured on to us, and we’re losing a lot of our normal community… because my friends passed away, my spouse passes away, my kids move away. And, what do we do best as recovering people? Community.
What are the needs of somebody who’s had a long-term history or struggle with addiction? Maybe they have special medical complications that are kinda unique to that niche group of folks.
So again, it’s one of those things that I never spent a lot of time looking into it, but I’ve always been kinda fascinated about it. We’re all getting older!