
Preface: I see a lot of change going on. Sometimes I like to take notes and get things down on paper in an organized way so I can clear my mind and try to make better sense of what I am noticing. This article is that. I share this writing for the sake of the idea that someone else might also be trying to make better sense of things as well.
My starting place is to back up to the idea of a helping relationship. A helping relationship consists of a helper and the one being helped. And that’s no different in the substance use arena.
A helper in the addiction arena might view addiction as either a disease, a disorder, a problem, or a symptom.

Meanwhile, the one seeking help might be on a path of whole-person long-term transformation, or seeking total diminishment of their disorder, or exploring options concerning mitigating use, or wanting an ally in their struggles.
When the helper and the one seeking help meet, I wonder if their individual understandings and purposes are a relative match?
And I wonder if we as addiction professionals steer those seeking help and our colleagues accordingly?
Changes in Understanding and Purpose
During the last few decades I have seen an expansion of research and clinical commentary about the nature of substance use problems and their associated helping methods. One result of this expanding effort I have noticed is the development and clarification of differences in how substance use problems are viewed among and between helpers and those seeking help.
And in more recent years, I have seen a rather vastly expanded discourse in academic, research, clinical, public health, policy and other arenas concerning the formulation of what moderate to severe substance use disorders are. What is especially interesting to me is that this development and clarification of differences is within the distinct category of moderate-to-severe substance use disorders – what would otherwise be called “addiction”. That is to say, within the category or concept of addiction, large differences have come to exist in how that more severe and specific problem is generally understood.
Likewise, I have seen a rather vastly expanded discourse in the same literature (and other sources as well) about the purpose of help as expected by and for those who are seeking help.
These differences in understanding addiction, the help being offered, and the help being sought, exist among helpers/helping systems on the one hand, and among those seeking help on the on the other hand. And so naturally there may be a relative match or mismatch of understanding and help between the helper and the one seeking help.
Differences in Understanding and Purpose
Addiction may be understood in vastly different ways. And those seeking help may be ready in very different ways. What are some possible identifiers within these differences? And what recent examples have you noticed?
Below I lay out a framework that shows addiction understood as a disease, or a disorder, or a problem, or a symptom. And for each of those I organize the clinical formulation of the helper and the functional readiness of the one seeking help.
Although working on this was somewhat of an academic exercise, working out this kind of thing helps me at times to organize and clarify what I am aware of.
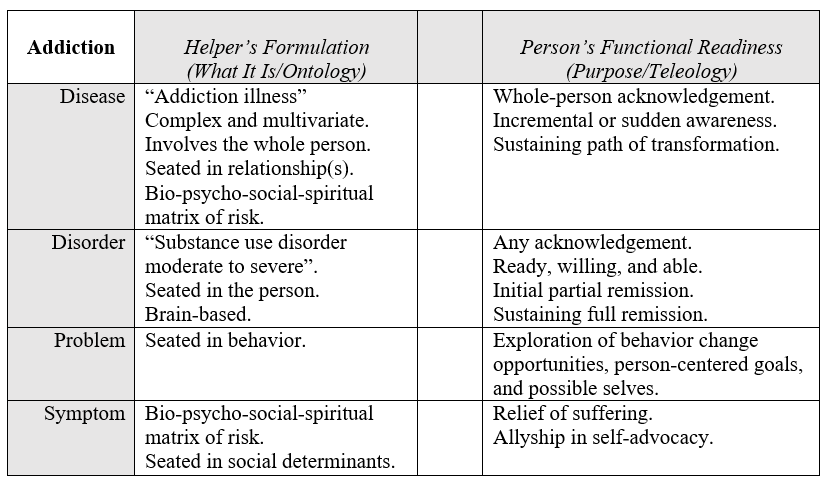
I’ll say a few things about some of the contents of that grid.
First of all, the open center column is supposed to hold the idea of “matching” like on a test in school. And it’s also meant to show the space within which the relationship happens. Really, what I have in mind is also “mismatching”, of course.
Another thing I wanted to clarify is that in my experience the clinicians that hold the disease model and those helpers more centered in social liberation are the most alike in one key way: the thoroughness of their general awareness.
Thus, I put “bio-psycho-social-spiritual matrix of risk” down for both of those views.
I say that as someone who was academically trained in hardline scientist-practitioner thinking, radical behaviorism, and cognitive-behavioral psychology. That is to say, I know all too well the comparative narrowness underneath the world view that sees addiction as a “disorder” or a “problem”. I will also say that as a result it is hard for me to be sure just how dispassionate I am in what I have included and not included in the grid, especially for the helper side of the “disorder” and “problem” categories.
The column on the right is about purpose, and I decided to add content in that column from the perspective of the person seeking help, rather than from the one providing help. I decided to do that in order to amplify the way a possible mismatch with the helper might manifest. And I decided to limit the content of that column to words centered in what that person might be seeking as well as their functional readiness. Far from complete, these are simple notes to help me clarify my own thinking.
Discontinuity
It occurs to me there may be a relative match or mismatch between the helper’s notion of what addiction is understood to be, and the purpose of the help as defined by the person seeking help. The space within the relationship of helper and person served may be improved or eroded by the fundamental assumptions each of them hold in this regard.
Further, the path or type of help sought by the one looking for help might shift, and this might improve or degrade the match over time.
Even more recently, COVID, various societal forces, and a significant increase in the USA of opioid overdose deaths seem to have collectively brought about a level of considering and reconsidering among many in our profession. And this has resulted overall in a relative stop, break, or discontinuity from the longstanding lineage, understanding, and historical context of our field.
I see the basic content, context, and lineage of understanding in our profession (as it has been seated in our historical continuity and shared in oral tradition, writings, and story) is eroding, And so, in the broader context of the professional part of our field, the former collective understanding of addiction and related helping is now relatively de-emphasized or removed.
And rather, at this moment in time, we are forming new ways of understanding and of helping that began and sit comparatively free-standing in time. It’s almost as if they were brought about and born in a space of discontinuity.
For example, the post-overdose response teams, needle exchange services, and overdose prevention efforts of today (as innovated in the current context) seem quite different to me from the needle exchange and prevention strategies I saw when I stated clinical work in 1988. And they have arisen very recently.
Forming Connections
I’ll leave the reader with some action items to consider that are framed as opportunities.
Rather than attempt to be all things to all people, we could remember to…
- …be more aware of emerging systems of help that are different or new.
- …be professionally and actively linked to newly emerging systems.
- …link helpers from other frameworks to those people they don’t know yet that work elsewhere within those kinds of spaces and kinds of help (so they can meet their peers).
Aside from the readings below, I’ll conclude by linking to an article summary; the reader might be introduced to a leadership style helpful in this context and worth investigating.
Suggested Reading
de Saussure, F. (1916, 1998). Course in General Linguistics. Open Court Classics: Chicago.
Levi-Strauss, C. (1958, 1974). Structural Anthropology. Basic Books.