Earlier in this series I covered the origin and early evolution of the Recovery Alliance Initiative, provided a description of the expansion and clarification of our model and methods, and outlined a recipe we uncovered of general similarities among effective sectors. I also described a stretch-goal for our field: attempting from the very start with each person to achieve full remission five years after the last clinical touch.
But how could these models and methods translate into something in real life?
In this post I’ll attempt to answer the question, “What do the practical elements of our Recovery Alliance model consist of and look like?” by concretely sharing our practical perspectives, as follows.
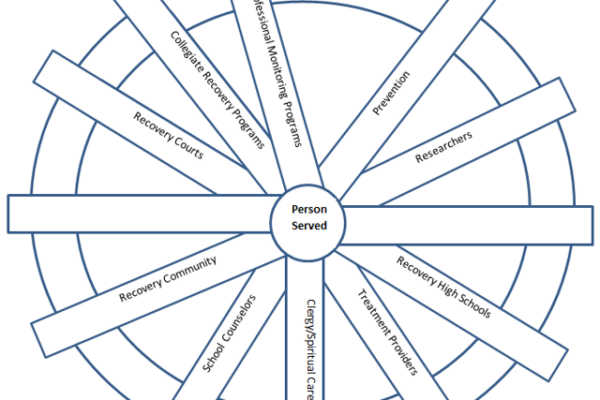
After we had added many more sectors to our original model that only consisted of three, Tom pushed me to make a visual diagram that showed the entire Alliance.
Here you can see the Recovery Alliance from a different perspective.
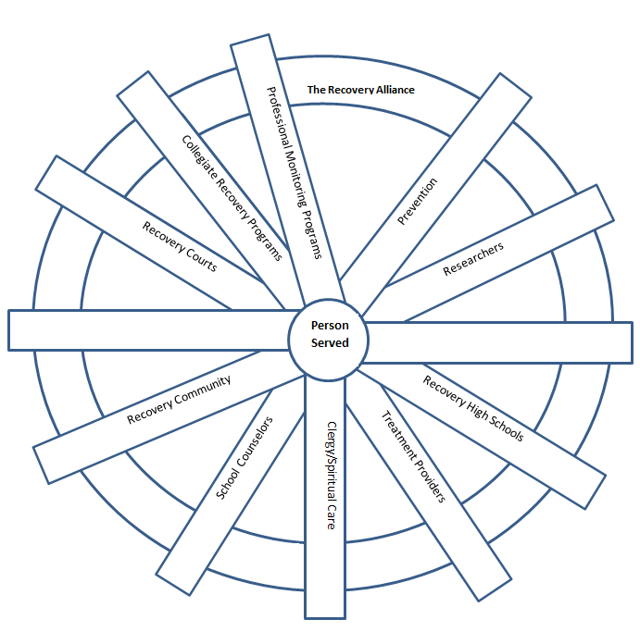
This simple artwork I created shows the person we serve as central, and the various sectors listed as spokes. We are always careful to keep some spokes blank, with no name written down on them. Why? Keeping some blank is a placeholder for us not knowing everything and for us still learning. In other words, we can add other sectors later that we don’t know about yet.
Further, when we come together as the Alliance in a Summit meeting, we form bonds that hold us together – represented by the wheel around the outside of the circle.
Tom then asked me to provide a visual example of one hypothetical person over time. So, I made this example, pictured below.
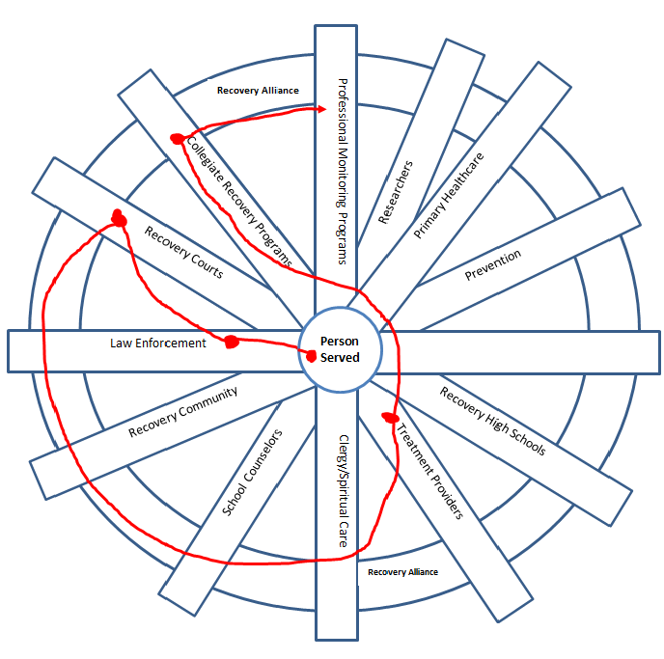
Here you can see the journey of an imaginary person who:
- was first arrested by law enforcement
- was next seen to be in need and shepherded into a drug court
- helped clinically by a treatment provider during their time in drug court
- started to imagine a new life such as going to nursing school
- was supported by a collegiate recovery program during nursing school, and
- finally entered professional monitoring when they pursued their license to practice.
All along the way the person was helped proactively with information, support, accountability, and advocacy both before and as their life situation improved and their personal goals unfolded.
Of course, you could make up any number of other examples that would all be very different. And you could adjust the path and particular sectors used with each individual person accordingly.
Next, I’d like to show you two other practical ways to look at this. One is up and down, and the other is across.
First let’s look at the up and down example using a diagram I made.
Imagine turning that wheel diagram we just looked at on its side. Then copy that diagram vertically a number of times. The result provides a perspective of the opportunity: to move up from the local level, one level at a time, toward the national level, or downward from any given level through specific levels toward the community level.
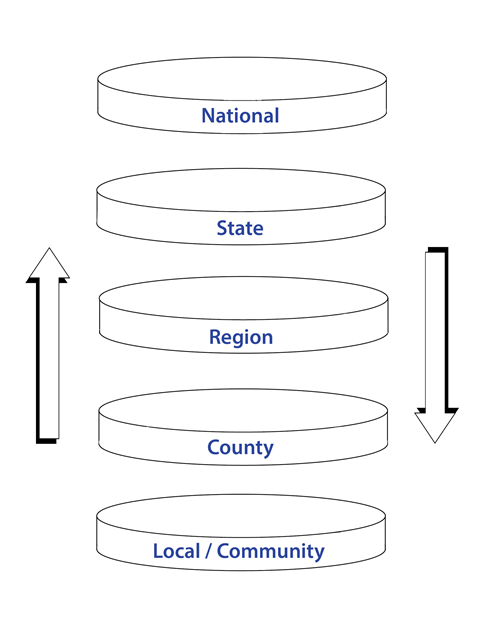
Here you can see systems like the ones we work in (the spokes) have a local presence but might also sit within a national organization or a national model. This is important to consider because it can help us to slow down and remember that there may be various resources (informational materials, directories, and people, etc.) that are plentifully available.
- We may find useful resources and people that can collaborate with us up and down the scale, and help the person served
- We can also receive and share with others in this way for the sake of system improvement.
Would it be helpful to examine a national directory, speak to a person in a different state, or check for a resource in the person’s local community? Have you done your own homework first to locate available resources, rather than merely assume certain resources don’t exist?
While we do this work in the Alliance we use a few key strategies to remain mindful of the intent of our effort. Toward that end we keep the principles of Behavioral Health Recovery Management (BHRM) in view. Those principles provide us a practical perspective of a different kind.
The BHRM principles are named below. I’ve included a link for a brief resource on the those principles. It is very readable; each principle is described clearly in a short paragraph.
- Recovery Focus
- Empowerment
- De-stigmatization
- Evidence-Based
- Clinical Algorithm
- Apply Technology
- Service Integration
- Recovery Partnership
- Ecology of Recovery
- Monitoring & Support
- Continual Evaluation
Here, I will provide the verbatim statement about the BHRM Principle called a “Recovery Focus”, in case the reader does not know the BHRM principle well and might make assumptions about what it means.
Recovery Focus: Full and partial recoveries from severe behavioral health disorders are living realities evidenced in the lives of hundreds of thousands of individuals in communities throughout the world. Where complete and sustained remission is not attainable, individuals can actively manage these conditions in ways that transcend the limitations of these disorders and allow a fulfilled and contributing life. The BHRM model emphasizes recovery processes over disease processes by affirming the hope of such full and partial recoveries and by emphasizing client strengths and resiliencies rather than client deficits. Recovery re-introduces the notion that any and all life goals are possible for people with severe behavioral health disorders.
So far in this post I have covered a practical perspective that is vertical. I would like to share another practical perspective I found and brought to our work in the Alliance. This perspective is within or across one of the vertical levels.
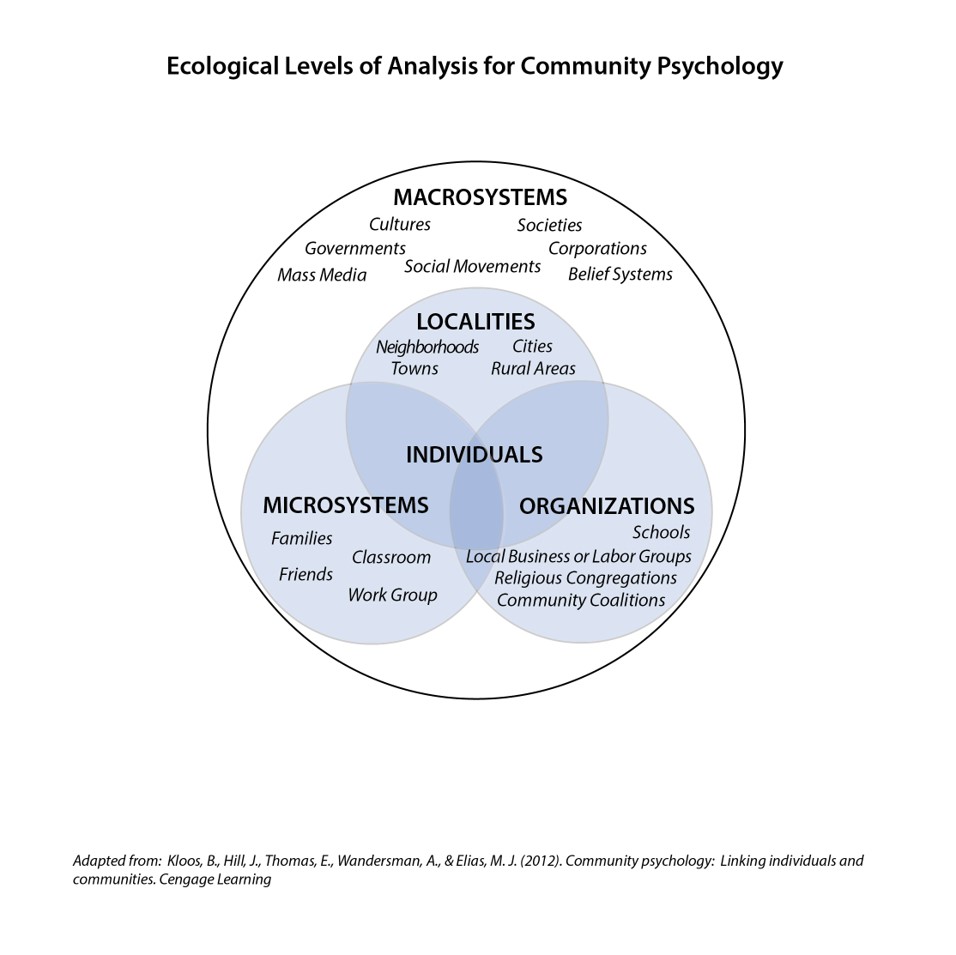
If you look at that diagram carefully and really consider it you can see where the person we serve sits within a community.
- Different communities have different kinds of spaces and resources.
- No one person and no one sector can think of everything, or do everything.
So, it’s good to consider the person from this kind of perspective. Adding this perspective may help move us towards being more effective, accessing available resources, and thinking of new and practical collaborations very specifically and locally.
Can we invade our spaces or such community spaces with improved awareness? Can we form collaborations with those serving within these sub-systems? Can we advocate within and for those serving within these macro and micro community resources? What actions can we take or support within these spaces to help the person served?
Struggling with questions like those led Tom (especially) to go further in his thinking and consider macro-level system change. He really did his homework on that topic and found an amazing resource. In the next post I’ll outline the resource he found. It’s a structured method that guides people in effectively making and sustaining large-scale systemic impacts.
What he found really inspired me so I went looking for myself. The next post will also contain the system change resource I found and hbave used routinely in much of my regular work outside the Alliance ever since.