This is the first post in a series within which I will provide an overview and history of the Recovery Alliance Initiative.
Here’s the Alliance website in case you would like to check that out.
The Recovery Alliance Initiative began as an idea in 2013.
What started as an idea developed into a structured method of bringing together divergent sectors within our field, and guiding them in:
- beginning collaboration across their differing systems
- developing awareness of needs for our field that remaining siloed would not reveal
- forming working groups to take on those needed improvements as formal change projects
- and simple cross-fertilization across their sectors
And in all of this, we work at keeping the effort centered in the sake of the individual person being served.
I’ve presented a good amount of this information at a variety of national, state, county, and other gatherings over the years. And I’ve published materials related to this effort in various forms. But this is the first time and place I’ll be directly covering the whole topic, across the entirety of the project’s lifespan, in writing. The last post in the series will include the list of references for this series and suggested readings.
Origin
The way the Alliance started is a story that to me personally is rather funny.
Tom Edwards, whom I know quite well and has worked in our field for decades, said to me on a phone call late one afternoon in 2013, “Collegiate recovery programs, and professional monitoring organizations – what do they have in common? Tell me why to put them in the room together.”
I really wanted to take time to consider that question and so I asked him for “…permission to think” before I answered. He granted me that permission.
Two weeks later I called Tom and said, “Hey Tom, do you remember that question you asked me?” He said he had no idea what I was referring to. I reminded him of the question he had asked and that he gave me “…permission to think.” He said, “Oh, yeah.” I said, “They’re the same person.”
He stated politely that it seemed I misunderstood his question. He clarified his question and again asked me what the different people served in those two systems had in common.
I put my reply to him this way: “Tom, they’re the same person. Someone who is a licensed professional today was a student yesterday. It’s the same person.”
He totally got it.
The subsequent conversation we had sparked a focused (and at times rather laborious and intense) collaboration between us that has lasted from that moment to the present day. (As an aside it’s worth pointing out that Tom and I are very different from each other in many ways, the least of which is not the fact that he is not a clinician.)
Based on the idea that continuity could exist between collegiate recovery programs and professional monitoring organizations, we planned to facilitate a gathering of leaders from those sectors.
In 2014 we invited some leaders from those two sectors, as well as some others that work with those patients, to meet at a gathering Tom and I would facilitate.
For this first gathering we focused on the national level. By “national level” I mean two things.
- We invited some people that functioned at the national level within their sectors.
- And we also invited leaders from those sectors that worked locally or regionally but were at the national-level in their knowledge and skill.
So that year we began to hold national-level summit meetings helping those two systems to meet and interact.
During our process of structuring and facilitating those early gatherings, Tom and I noticed key cultural and practical differences between the collegiate recovery and professional monitoring systems. While we facilitated the attendees through our process the differences between these systems emerged and became quite clear. This became rather awkward for us and for some of the attendees. And the process Tom and I were facilitating at times became somewhat difficult for us to manage. Tom and I were less prepared than we thought we needed to be.
I’ll say more a little later about some of the major differences between those systems that emerged during that process.
Tom and I learned a lot of things on a lot of levels from our facilitation of those early Summit meetings. Part of what we learned included how we would go about things differently.
Largely in response to the differences that emerged, I made and attempt to learn and took on a fair amount of reading. Within the next year or two I read a rather large amount of literature examining the theory, method, evaluation, and effectiveness of those two very different systems. I also read related book chapters, monographs, peer reviewed review articles, and so on.
Next, having done more than a little reading, I started to do some professional writing on the topic. In that process I was helped in my clarity and focus by another challenge Tom gave me. He said, “People like visuals. Turn your main idea into a visual diagram.”
For me that was hard. I’m often a visual thinker, but not so for this. All I could come up with at the time was one simple visual model that seemed unimpressive to me. I sketched it and gave that drawing to someone who does visual layouts for us. I showed the final art work to Tom. It was simple enough that he liked it. I was surprised. Here it is.
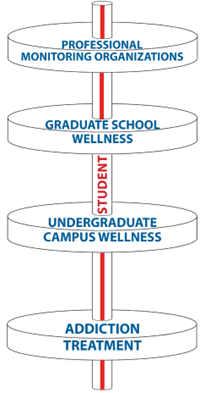
The image above includes a number of ideas. Here are a few of the main ones.
- The person served is central to our purpose.
- Relative to our systems, the person has a long timeline (upward) of their personal life.
- The top of the system is open, connoting in-flow and a relatively green ecology.
- I wanted to show the potential of long-term support being available over time.
- I also wanted to show the caution or problem of unnecessary gaps.
During our Summit meeting we had the sector leaders describe their philosophies and operational methods to each other. The cultural divide between these two kinds of systems was shown to be very wide. As the different sectors shared, the content at times was difficult for the attendees from the other system to receive. And for Tom and me the process of promoting mutual education and formation of support across these systems was at times difficult to facilitate. The divisions were quite real.
I wrote up the essence of my thinking and published an article in 2015. If you’re reading this blog post, I would encourage you to read that article (Coon, 2015).
Part of what I covered in that article were the cultural and practical differences Tom and I came to discover that exist between those two systems. For example, I described that the emphases of accountability and advocacy were generally reversed in their order of priority between those two systems.
- For collegiate recovery programs (CRP’s) advocacy is central, and the program can also include accountability secondarily, as needed.
- But in a professional monitoring organization (PMO) accountability is relatively central, and advocacy can eventually come about as a result.
In my next post in this series, I’ll describe the early evolution of the Alliance. That will include a description of how we clarified and improved our method at bringing numerous and disparate specialty sectors in our field together. And it will cover how we went about helping those sectors form mutual and collective collaboration and advocacy.