Prevention of substance use is probably more important than ever. And the relevance of prevention across the lifespan (including among those who have already initiated use) has probably never been more important.
Why would I say that?
The purity and potency of substances have increased so much that preventing even a one-time use of certain chemicals can now preserve the quality of life and be lifesaving work.
It now seems to me that Prevention should:
- be a service within every stage and level of care
- apply continuously across the lifespan, and
- no longer be a stage and kind of care that only happens before first use.
And it seems to me that all existing Peer Support and Harm Reduction specialists should be cross-trained in Prevention. (In that way we would not create the burden of adding Prevention-specialist staff to all services).
Why we all need to learn prevention
The new problems related to availability, potency, and addiction potential associated with:
- fentanyl, sufentanil, carfentanil, and novel high-potency opioids (e.g. causing death upon the very first use),
- novel high-potency benzodiazepine derivatives (e.g. causing complicated and hard-to-manage withdrawal; seizures; prolonged confusion after stopping use),
- novel high-potency methamphetamine derivatives (e.g. causing prolonged paranoia, irritability, and problems with decision making and impulse control lasting long after cessation of use), and
- ultra-high potency THC formulations (e.g. prompting onset of first psychosis; and psychotic episodes lasting days, weeks or months after cessation of use);
are serious and concerning.
In addition to the problems listed above, those illicitly selling substances now commonly add very high potency pharmaceuticals and novel synthetics to the street-level supplies of both prescription medications and “natural” drugs. Thus, today, one’s first use may no longer be to merely “try pot” but rather to “vape high-potency THC wax” – and accidentally die of an opioid overdose from the fentanyl the person did not know was in it.
The clinical presentations of these problems I have seen in recent years are dramatically worse than the problems associated with potency I saw in addiction treatment in the late l980’s through the 1990’s.
- Prevention should be added as a service within and across every stage and level of care.
- Prevention should apply across the lifespan.
- Prevention should no longer only be a stage and kind of care before first use.
- Existing specialists in Peer Support and Harm Reduction should be cross-trained in Prevention (rather than add Prevention-specialist staff to all services).
Classic Versions of Prevention
Prevention has typically focused on maintaining the prohibition against initiating substance use. This work has typically been focused on children and adolescents.
In that way, prevention was usually thought of as only happening before any use begins, and before harm reduction efforts are relevant. This is especially true when considered chronologically, or across the segments of a person’s lifespan.
That approach retains merit. Perhaps the simplest first reason to prevent initial use is what I have called the Harms of Use. For example, research efforts to quantify and scale:
- the wide variety of simple harms of simple use1
- physical harms, physical dependence, and social harms from substance use2
- genetic vulnerability to both simple harms and to addiction potential3, 4
- vulnerability to developing a substance use disorder based on the facts and circumstances of one’s life (e.g. Adverse Childhood Experiences), and
- years of life lost5
have been undertaken.
When I entered clinical work in addiction treatment back in the late 1980’s, the average addiction counselor I met knew that Prevention programs existed. But almost none of the addiction counselors I met seemed to know any specifics about what was done by the workers concentrating in Prevention.
At that time, Prevention as a field generally:
- centered on child and adolescent populations
- focused on primary prevention (preventing initial use)
- did its work in non-clinical settings (e.g. schools)
Prevention work was largely concerned with:
- promoting psychosocial health (e.g. self-esteem) and improving resiliency – as matters related to decreasing the numbers and rate of youth initiating substance use
- preventing initial use in the first place, especially among those for whom risk factors of SUD disease progression were present.
In that way, Prevention did not apply during active addiction illness, nor impact the course of addiction illness once the illness began.
Is that approach to Prevention sufficient today?
Classic Versions of Harm Reduction
Harm reduction (HR) in its classic formulation is centered in providing education, supplies, and related methods for safer use among people who already use substances or are experiencing addiction illness over a longer term. In that way, harm reduction is centered in lowering the negative effects of use. HR efforts can be implemented with:
- those who are experiencing simple use (and not a substance use disorder),
- for those with a mild use disorder, and
- those experiencing complex, severe, and chronic addiction illness.
During the late 1980’s, seemingly all the counselors I worked with or met knew about Harm Reduction approaches generally, including:
- the needle exchange and related education services we had in our city (that the Police in town knew existed, but did not target)
- the outpatient methadone maintenance program in town (which began operation in the late 1960’s, and I worked in for many years), and its graded responses to opioid use and use of other substance classes – such as cannabinoids or alcohol during methadone maintenance
- that the 1-2 year residential program (Therapeutic Community model) in town did not necessarily administratively discharge patients for alcohol use while on pass during the final (re-entry) phase of treatment
- the axiom that “We don’t kick the patient out of the respiratory ward for coughing.”
Is that Harm Reduction approach sufficient today?
A New Look at Some Old Ideas
Given the dangerously increased potency of many chemical compounds available today (especially compared to substances available when I started clinical work in 1988), some notions about the safety of use might be reconsidered. For example:
“Gateway drugs” is the common term for the idea that use of some less stigmatized substances opens the door to use of other drugs. The old idea of “gateway drugs” as a major concern has been challenged more recently as not so serious after all. For example, some newer thinking is that experimental substance use can be a normal rite of passage especially among young people.
- But laissez-faire attitudes about general experimentation with substances might no longer apply so widely, and might now depend on the specific substance of concern.
- For example, I ask myself “Today’s potencies are a gateway to what – an early death?”
“Chemical hooks” is a newer name for the drug effects like euphoria and craving that increase as potency increases. The idea of “chemical hooks” has been widely challenged more recently. And it has nearly been replaced with an alternative explanation of why people become addicted: Adverse Childhood Experiences.
- But failing to appropriately recognize dramatically higher potency might not properly factor in some relevant contributions of addiction-related morbidity and mortality being faced today.
- And I wonder, “Are ultra-potent formulations really not compelling in their impact?”
Given the commonly catastrophic harms (impacts) of even a single use of certain compounds, it seems to me that today Prevention, Harm Reduction, Peer Support, and Recovery Coaching should be components of one discipline.
And it seems to me that the aims of each of these individually are not diametrically opposed, but are in fact shared:
- Increased quality of life
- Decreased harmful impacts of use
Does Prevention become irrelevant during addiction treatment or during recovery from addiction illness? No – prevention remains relevant.
Prevention efforts that happen during one’s active addiction illness could prevent the initial use of a new and dangerous substance, as well as the related impacts (e.g. opioids and death from a single one-time use, or cigarettes and death after years of slow demise). Does Prevention become irrelevant during active addiction illness? No – prevention remains relevant even then.
Prevention, Adults, and Older Adults
Generally, our previous model of prevention made efforts before initial use, was aimed at the young, and was certainly undertaken before any disordered substance use. But that Prevention model also generally missed opportunities with those experiencing an onset of use late in life, those retiring, or those that lost a spouse.
Recent changes in society (at least within the USA) add stressors to our social system and to us individually. Our collective and individual adaptations may work for or against our interests in the short term or longer term. Compounding the pressure is the SARS-CoV-2 pandemic.
Consider the importance of “Prevention” in that context and in the face of these findings6:
- Early retirement is risk factor for mortality
- Prolonged working life may provide survival benefits
- 1 year older at retirement = 11% lower risk of all-cause mortality independent of sociodemographic data, lifestyle, and health confounds
- Unhealthy retirees have lower all-cause mortality when retiring later.
Looking Forward
Newer models of SUD services have emphasized implementation of:
- harm reduction strategies,
- innovation of new harm reduction approaches,
- harm reduction strategies as an outreach and stabilization method,
and may be followed by formal treatment. But those efforts have generally missed opportunities related to tertiary prevention and those late in the course of illness.
Historically, across the USA, provider organizations helping those with serious and complex addiction illness have arisen from motivated non-professional helpers, rather than formal systems of clinical care. That has resulted in both strengths and weaknesses within systems of care.
More recent empirical examinations of older methods like the DARE program and the still widespread clinical practice of ignoring cigarette smoking during addiction treatment have demonstrated opportunities to improve.
I suspect the current stressors in our society and in our systems of care for substance use disorders will result in problems that indirectly help bring about an improved model that will include:
- Training and service provision that is more like dentistry (a whole and unified model, comprised of wellness, prevention, and treatment with all methods available, across the lifespan)
- Harm reduction and Prevention as twin methods both available in all services and levels of care.
- Less opportunity for helpers to inaccurately project their own personal or professional experience as the proper method or path for the person served.
Some Personal Reflections
Having worked in a long-term (9-12 month) residential program:
- prior to and during that program’s initial shift to gender-specific care for women, and
- during its initial specialization to serving pregnant, post-partum, and parenting women (including having infants and children up to age 4 living with their mothers during treatment) – and
- doing the work of those specializations for the following 17 years,
I have a certain level of awareness and sensitivity to the topics in this essay as they pertain to prevention and the lifespan – to say nothing of the new problems caused by unprecedented potencies.
Later in those 17 years I undertook some personal study in developmental neuropsychology7, 8. In doing so I came to appreciate the basic biology related to cells differentiating after conception into neurons, and those neurons later migrating, developing and sub-specializing within the human physical system.
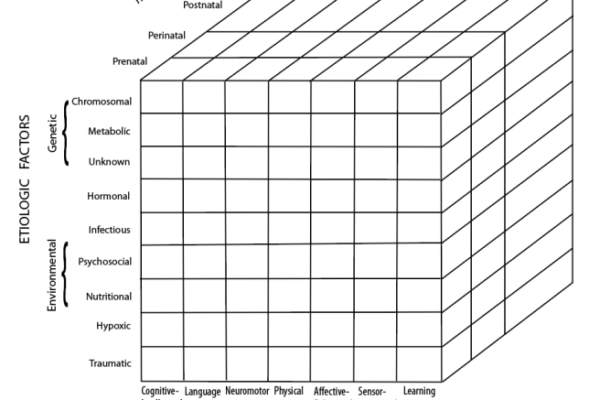
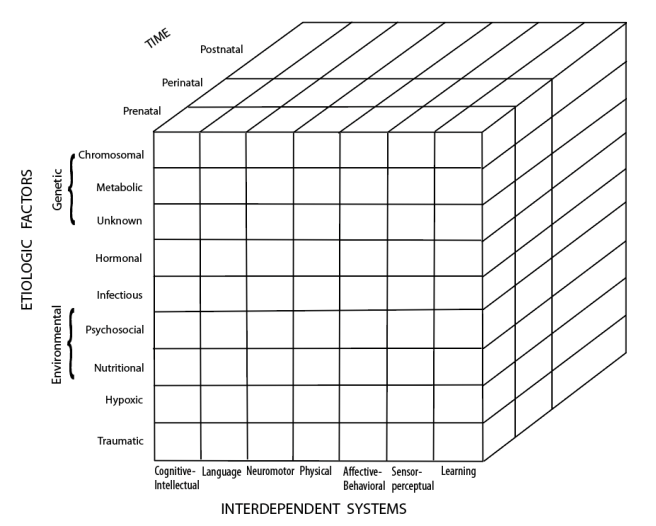
The diagram below, called the “Developmental Disabilities Cube”8, summarizes the major relevant domains of neuropsychological development and function. Think about today’s ultra-high substance potencies and the possibility of prevention across the lifespan as you consider this diagram.
Developmental Disabilities Cube
For me, witnessing over 17 years of:
- pregnant, post-partum, parenting women entering residential addiction treatment (many bringing an infant or toddler in to live with them during treatment);
- women returning to the program from the hospital after delivery of their infant;
- infants then entering the building to live with their mother during her stay;
- the results of developmental and functional assessments with those infants shortly following their birth and throughout the mother’s stay;
- the results of the targeted developmental interventions we conducted where some lags might have been present;
and outpatient methadone maintenance for 19 years
gives me a certain kind and range of clinical experience from which I can draw memories of patient narrative and case data. Those experiences help me have first-hand examples of various interactions between the causal factors and interdependent systems pictured in that diagram.
I have two suggestions to modify the diagram for our work:
- add clinical substance-related prevention techniques as an etiologic (protective) factor on the left-side vertical list;
- add segments of the entire life span (infant, child, adolescent, adult development and aging) after the “postnatal” phase at the back of the diagram.
References
1 https://recoveryreview.blog/2019/10/24/harms-of-use-a-list-of-references/
2 Nutt, D., King, L. A., Saulsbury, W. & Blakemore, C. (2007). Development of a Rational Scale to Assess the Harm of Drugs of Potential Misuse. Lancet. 369: 1047-1053.
3 Mazea, I. & Nestler, E. J. (2011). The Epigenetic Landscape of Addiction. Annals of the New York Academy of Sciences. 1216:99–113. doi:10.1111/j.1749-6632.2010.05893.x
4Verhulst, B., Neale, M. C. & Kendler, K. S. (2015). The Heritability of Alcohol Use Disorders: a meta-analysis of twin and adoption studies. Psychological Medicine. 45(5):1061–1072. doi:10.1017/S0033291714002165
5 Hall, O. T., Hall, O. E., McGrath, R. P., & Haile, Z. T. (2019). Years of Life Lost Due to Opioid Overdose in Ohio: Temporal and Geographic Patterns of Excess Mortality. Journal of Addiction Medicine. Open.
6Wu, C; Odden, MC; Fisher, GG & Stawski, RS. (2016). Association of Retirement Age With Mortality: A population-based longitudinal study among older adults in the USA. Journal of Epidemiology and Community Health. doi:10.1136/jech-2015-207097
7 Horton Jr., A. M., Ed. (1990). Neuropsychology Across the Life-Span. Springer Publishing Company: NY.
8 Spreen, O., Risser, A. & Edgell. (1995). Developmental Neuropsychology. Oxford University Press: NY.
Suggested Reading
Ciccarone, D. (2019). The Triple Wave Epidemic: Supply and demand drivers of the US opioid overdose crisis. International Journal of Drug Policy. doi.org/10.1016/j.drugpo.2019.01.010
Lewera, D., Tweede, E. J., Aldridgea, R. W. & Morley, K. I. (2019). Causes of Hospital Admission and Mortality Among 6683 People Who Use Heroin: A cohort study comparing relative and absolute risks. Drug and Alcohol Dependence. 204. 107525. doi.org/10.1016/j.drugalcdep.2019.06.027
Acknowledgement
Thanks to B. Schlosser for the artwork preparation of this representation of the Developmental Disabilities Cube.