
Chapter excerpted from the upcoming book:
ADDICTED IN FILM
Movies We Love About the Habits We Hate
(And How They Can Help Anyone Recover Successfully
and Lead a Happier Life)
by Ted Perkins, facilitator and “Tips & Tools Guy”
Reserve your copy today!
100% of all future proceeds, from any Bookshop sales, will be donated to support SMART Recovery.
Note: this review of Dopesick TV series expresses the opinion of Ted Perkins only, and is not intended to express the views of SMART Recovery as an organization.

I’m the first guy to tell you that movies and TV shows are a business first and foremost, which is why most screenwriters and producers like me strive to make them as provocative, romantic, comedic, horrifying, and/or thrilling as possible. Unfortunately, many media critics bemoan the negative impact of commercial imperatives on “quality” storytelling, and why Marvel superhero franchise films usually take the brunt of the criticism. But Hollywood is also known to take chances from time to time, and some of its greatest artistic and public-service accomplishments have occurred when it dramatizes important current events. Hulu’s original series DOPESICK is a prime example of how producers endeavored to take on a difficult and challenging issue like the opioid epidemic and hit it out of the park.
It must have been no small undertaking. The now well-documented and exhaustively researched story of how Purdue Pharma and the Sackler Family managed to flood the country with a highly addictive pain medication like OxyContin could fill volumes. For an in-depth look, I highly recommend Patrick Radden Keefe’s bestseller Empire of Pain: The Secret History of the Sackler Dynasty. HBO also produced a powerful documentary on the subject called The Crime of The Century. These two dispassionate takes on the story are vital to the national discourse on the topic, but with DOPESICK the producers have managed to give this complex story a deeply human, very emotional dimension.
DOPESICK tells the OxyContin story from several different vantage points—from the coal mines of West Virginia to the Boardrooms of Purdue Pharma to the halls of the FDA. The story is anchored around no-nonsense country doctor Samuel Finnix, played by Michael Keaton, in a role for which he won the 2022 Golden Globe Award for Best Performance by an Actor in a Miniseries. If you haven’t seen his acceptance speech, I highly recommend you watch it on YouTube. The series itself is an emotional rollercoaster as it is; Keaton’s speech in real life takes it to a whole other level.
Finnix is an everyman good guy family practitioner who dotes over his low-income patients in a small West Virginia mining town. Many come in for help with the injuries and the associated chronic pain caused by hard physical labor in the mines. One of them is Betsy, played by Kaitlyn Dever, who suffered a back injury. Her physical pains are further compounded by the emotional stress of keeping her sexuality a secret from her Christian parents and community. Writer/Producer Danny Strong made a wonderful decision to humanize Betsy in such a way that her subsequent fictional addiction to OxyContin is caused by a multiplicity of factors (physical and emotional), just like addiction is in non-fictional real life.
Betsy’s injury just happens to (unfortunately) coincide with the rollout of a new “miracle drug” pain medication called OxyContin. Finnix learns about it when he receives a visit from a polished drug sales rep named Billy, played by Will Poulter. Billy’s the pride of the Purdue Pharma sales and marketing department, a boiler-room that thrusts young and eager 20-something overachievers into every doctor’s office in America to sell a lie: OxyContin isn’t addictive. While Finnix has enough common sense and medical knowledge to doubt this spurious claim, Billy’s sales pitch does sound pretty compelling. So, he writes Betsy a prescription for her pain. And to test OxyContin out for himself, he tries one (but just one) pill from the countless free samples Billy leaves behind as promotional freebees. You can guess where this is going.
The story then rewinds a few years to show the architect of all the ensuing misery, Richard Sackler, played with surreal creepiness by Michael Stuhlbarg. Somewhat miraculously, the writers have managed to humanize one of the most despicable characters in recent memory. Sackler comes off as a sad rich kid overshadowed by the achievements of his father and grandfather. OxyContin—a new “blockbuster drug” —is his desperate attempt to earn his family’s love and respect. So, what if, for him to earn his gold star, it’ll endanger and destroy the lives of hundreds of thousands of people? Ah, the banality of evil.
What is so striking about DOPESICK is the way the story goes on to portray the complexity of how Sackler and his Purdue Pharma foot soldiers cleverly managed to manipulate, dupe, and/or bribe seemingly respectable doctors and medical opinion leaders into endorsing a product that even a first-year medical student could have told you would be highly addictive. Purdue even put one over on the FDA to keep OxyContin off the list of heavily controlled substances. Equally fascinating (albeit horrifying) is how Purdue’s sales teams continually doubled down on the lies told by their sales reps every time anyone raised a red flag. And if that didn’t work, they just doubled and quadrupled the dosages per pill in order to combat “Breakthrough Pain,” a made-up medical condition that was really just users building up a tolerance to the drug and needing higher and higher dosages so they wouldn’t get dopesick. Talk about pouring gasoline on a fire.
With Sackler and Purdue firmly established as the ultimate Goliath, the story then introduces us to the Davids, no-nonsense country lawyers Richard Mountcastle (the always amazing Peter Sarsgaard) and Randy Ramseyer (John Hoogenakker). Their slow and methodical search for the truth, and their crusade to bring Purdue and the Sacklers to justice, plays out like an Agatha Christie mystery crossed with Erin Brockovich. To call these two guys “heroes” is an understatement, both in the series and in real life. Mountcastle gives up any semblance of a personal life during his decades- long investigation. Ramseyer even goes so far as to refuse to take OxyContin to relieve the pain of his prostate cancer surgery. Not because he thinks he’ll become addicted, but because it would put more blood money into Richard Sackler’s pocket.
Equally heroic is Bridget Meyer, a scrappy and ambitious DEA agent played by Rosario Dawson. Dawson does a superb job of looking calm and collected (albeit indignant) as the OxyContin catastrophe unfolds in plain sight all around her. Her sclerotic agency seems to be too afraid of intergovernmental red tape to do much about it, and she gets stonewalled at the FDA—an agency seemingly beset by an admixture of dark money influencers (mostly funded by Sackler) and unscrupulous regulators (many of whom went on to cushy six-figure jobs at—you guessed it— Purdue Pharma!).
As the conspiracy investigation unfolds, we eventually circle back around to Purdue’s primary victims in the story, Dr. Finnix and his patient Betsy. Her well-intentioned effort to use OxyContin “as prescribed” for pain quickly spirals out of control. She’s reduced to turning tricks in seedy back alleys after she loses her job for being high. Overly dramatic made-for-TV overkill? Not at all. Betsy’s fictional story is similar to that of many people swept up in the opioid crisis in real life. Most had jobs, were well-educated, had families, paid their taxes, walked their dogs. The farthest thing from their mind was to become addicted to drugs. Problem is, they had pain. Real physical pain. And for that they simply wanted help. But they got something else.
Finnix (Michael Keaton), the one guy you’d think would know better, quickly gets consumed by the drug as well. Desperate for money, he gets recruited into the Purdue Pharma “Speakers Series”—basically Ted Talk for OxyContin apologists and liars. All he has to do is step in front of the mike, say he’s an MD, and tell everyone the drug isn’t addictive. And all of this as he himself is addicted and high as a kite. Granted, Finnix is a fictional character, but his path to the “dark side” mirrors that taken by countless other once-respectable medical professionals who the Sacklers bought off to help them overcome critics and move more inventory.
What makes DOPESICK especially relevant to the overall conversation about recovery is just how difficult it was for treatment providers and mutual support groups to combat such an addictive drug. Betsy white-knuckles it at 12-Step meetings and attends group prayer at her church. But neither NA nor the Almighty seem to be any match for Purdue Pharma’s “miracle pain reliever.” While Narcotics Anonymous may have helped some individuals overcome their addiction, in Betsy’s case her meetings turn out to be secret OxyContin swap meets. (I have reached out to long-time SMART Recovery facilitators to see what their experiences were with meeting participants struggling with OxyContin addiction at the time.)
Finnix, meanwhile, loses everything, including his medical license. He goes to a rehab facility. However, like many people legally mandated into recovery, his initial (defensive) reaction is to feel like an outsider. He’s not addicted like “those people,” no sir. What’s worse, he realizes that many of the other patients at the facility have cycled through several times before. Whatever it is that’s supposed to be “working” in this rehab facility clearly isn’t. But that could be said about many rehab facilities at that time. When it came to the fight against OxyContin, literally everyone in the recovery universe seemed to be boxing outside of their weight class. Such was the power of this drug. Finnix eventually leaves the facility, relapses, then seeks recovery help at a methadone clinic.
DOPESICK culminates in Mountcastle and Randy Ramseyer’s successful prosecution of Purdue’s deceptive marketing and business practices. This eventually led to Purdue’s bankruptcy and multi-billion-dollar settlements (still in contention today). It’s a satisfying ending to a sad story, but in many ways it’s cold comfort. It took the U.S. judicial system more than a decade to put a halt to a tragedy that was blatantly obvious to anyone who cared to look. Thousands of people died needlessly. Entire communities were ravaged. All while the Sackler family made billions. So, was it just the Sacklers’ fault? Well, yes and no.
DOPESICK lets us peel back the curtain and see all the moving parts of this consumer product catastrophe. It was a perfect storm of contributory negligence. Purdue’s chemists knew the drug was highly addictive, so they bribed medical professionals to say it wasn’t. They submitted skewed data sets with sampling errors to regulators, whose job it was to know better. Purdue’s legal team knew they would never pass muster with the FDA, so they rewarded the FDA chief (Curtis Wright) with a $400,000 a year job at Purdue if he would help them create a loophole. Purdue’s marketing department knew the drug was addictive, so they paid users to say it wasn’t in promotional videos. Purdue’s sales department was under pressure to meet its targets, so they offered ridiculous commission structures to motivate its avaricious young sales teams. Yes, everyone at Purdue could say they were “just following orders.” But that didn’t work at Nuremberg, so why should it work here?
Not surprisingly, we see money at the root of this evil. A perverse amount of money. The financial incentives created by Purdue to market and sell the drug cascaded down the value chain. Small private pharmacies could mark up OxyContin and make higher margins on its sales (but in all fairness, they were also afraid that Purdue would sue them if they didn’t sell the pills). Medical and treatment professionals with prescription privileges stood to make a lot of money too. After all, they were helping people manage chronic pain, right? And thus, the infamous “Pill-Mills” formed around the country. Watchdog groups could reap millions in off-the-books “sponsorship” revenue from Purdue if they looked the other way. If all of this doesn’t smack of a criminal conspiracy, what does?
By revealing the interdependence of all these bad faith actors, DOPESICK does a wonderful (if maddening) public service. It illustrates how actual conspiracies work. How criminality is allowed to fester in plain sight because it seems too outlandish to believe it’s actually happening (I’m reminded of the quote attributed to Edmund Burke: “The only thing necessary for the triumph of evil is for good men to do nothing”). This situation demonstrates how a lie told enough times eventually becomes the truth. And if that doesn’t work, just pay more people more money to parrot your talking points. These are painful lessons society seems to have to relearn over and over
again.
I also think DOPESICK is an important series to watch because it’s an unflinching look at addiction in general. Both what addiction is, and what people think and say it is. OxyContin is a case study in how real societal harm and death is caused by the language we use to describe and stigmatize individuals who suffer from addiction. We often hear in church, “Love the Sinner; Hate the Sin.” Well, the Sacklers made billions and avoided criminal prosecution by just flipping the sentence around: “Hate the addict, love the addiction.” OxyContin was harmless. The Sacklers were innocent victims of a vast left-wing anti-business conspiracy. It’s all the “pill-heads’” fault. Sound crazy? No, not at all. The Sacklers were just channeling the idea that addiction is a moral failing, completely unmoored from any physiological or mental health considerations. This idea is out of date, it’s wrong, and it’s killing people. SMART Recovery’s been saying this all along and will continue to say it as part of its support of Harm Reduction. Luckily, public views on addiction are slowly changing thanks to groundbreaking work by scientists like Dr. Nora Volkow (recently featured in a SMART Recovery webinar).
While DOPESICK spreads out culpability for the OxyContin Opioid Epidemic among many participants and institutions, I’m reminded of something my father once told me: “The fish rots from the head down.” And in my mind, that rotten head was Richard Sackler’s. He was the architect of the drug, the crimes, and the coverup. To date, he and his minions have avoided criminal prosecution in exchange for billions in civil settlement fines. As you read this, these settlements are still under review and appeal. On the one side, victims are demanding personal accountability from the Sacklers; on the other, states desperately need that settlement money to help clean up the mess they made. The Sacklers recently participated in a court proceeding where family members of OxyContin victims were allowed to confront their tormentors. Richard Sackler joined via Zoom, but only because he was forced to. His camera was turned off.
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!
Avoiding Complacency
Whenever we accomplish something, we naturally feel excited and proud of ourselves. After leaving treatment, those in recovery are especially proud – they have just dedicated time and effort towards self-improvement and making lifestyle changes. However, recovery is not a “one and done” achievement – it is something to constantly work towards, which is why addiction is known as a chronic disease.
When first leaving treatment and during the e arly recovery period, people feel empowered and strong in their recovery, happy about all they have accomplished. They may feel they are at a point where they can take a break and remove recovery from the top of their mind. This leads to complacency. Complacency is defined as “self-satisfaction, especially when accompanied by unawareness of actual dangers or deficiencies.” Here are a few common reasons why people become complacent in their recovery – along with strategies on how to avoid complacency and focus on long-term recovery.
arly recovery period, people feel empowered and strong in their recovery, happy about all they have accomplished. They may feel they are at a point where they can take a break and remove recovery from the top of their mind. This leads to complacency. Complacency is defined as “self-satisfaction, especially when accompanied by unawareness of actual dangers or deficiencies.” Here are a few common reasons why people become complacent in their recovery – along with strategies on how to avoid complacency and focus on long-term recovery.
- Don’t ride the pink cloud – Most people in recovery have heard of, or experienced, the “pink cloud” – a period within early recovery where a person feels euphoric, proud, and excited. There’s nothing wrong with being positive and optimistic after achieving a goal, but the pink cloud can take over and make you avoid facing the reality of long-term recovery as you “float” above the world, forgetting about real challenges in recovery like navigating work, relationships, and aftercare. Use your early recovery period to build a plan for tackling these long-term issues instead of riding the pink cloud, and you’ll already be a step ahead.
- Don’t lose sight of the bigger picture – Early recovery is important, but it is only part of the journey. Focusing too heavily on early recovery can cause you to lose sight of your end goal, which is maintaining recovery over a long period of time and incorporating recovery into your everyday life.
- Keep up with the program – After 90 meetings in 90 days, you may feel like it’s time to relax. Many people return to use after 90 days because they feel like they have their addiction under control by that point. Attending meetings and keeping in touch with your sponsor are crucial to successful recovery. Without that constant support and reinforcement, it’s easy to trail off into relapse.
- Continue to be of service to those in your recovery network as well as your community. Giving back is a main tenet of the 12 Step Program because it allows you to feel good about yourself and help those around you, all while keeping recovery a priority. Again, keep long-term goals in mind, like becoming a volunteer or program speaker after a year of sobriety.
It is all too easy to fall into the trap of complacency once you have exited the early recovery period. As long as you continue to make recovery a priority, and stay connected with those in your support network – as you did while you were in treatment and early recovery – your chance of sustaining successful, long-term recovery greatly increases.
***
For more information, resources, and encouragement, “like” the Fellowship Hall Facebook page and follow us on Instagram at @FellowshipHallNC.
About Fellowship Hall
For 50 years, Fellowship Hall has been saving lives. We are a 99-bed, private, not-for-profit alcohol and drug treatment center located on 120 tranquil acres in Greensboro, N.C. We provide treatment and evidence-based programs built upon the Twelve-Step model of recovery. We have been accredited by The Joint Commission since 1974 as a specialty hospital and are a member of the National Association of Addiction Treatment Providers. We are committed to providing exceptional, compassionate care to every individual we serve.
| National Drug Court Month Week 1 Recap As the first week of National Drug Court Month concludes, we are overwhelmed by the incredible headlines of hope and recovery from across the country. Treatment courts from coast to coast are sharing their stories of lives saved and communities transformed, holding graduations and community events that build public support. We’ve also been impressed with the powerful submissions to our Art of Recovery contest. To learn more and submit your work, click here. |
| The Bureau of Justice Assistance touts 30 Years of treatment courts: “Justice Reform That Works” BJA published a remarkable blog post highlighting the enduring success of treatment courts and the crucial role of the Drug Court Discretionary Grant Program in helping the movement thrive. The piece quotes BJA Director Karhlton Moore saying, “One of BJA’s great strengths is supporting innovative local programs and then spreading the lessons learned from them around the country. BJA programs promote fresh thinking and new experiences, and then help these insights achieve widespread acceptance and adoption. Drug court is a terrific example of how this process works.” |
| Chief Justices from Nebraska and North Carolina issued proclamations declaring May National Drug Court Month Said North Carolina Chief Justice Paul Newby: “North Carolina’s treatment courts have been working to restore lives and families for 27 years. We set aside this month to raise awareness that treatment courts can help break the cycle of addiction and crime and encourage hope and healing through recovery.” |
| Hawaii’s Kona Drug Court team visits and thanks businesses hiring treatment court graduates In this unique celebration, Hawaii drug court Judge Wendy DeWeese toured local businesses and learned how they help individuals in recovery. Judge DeWeese thanked business owners for not giving up on treatment court participants and alumni, saying, “It’s really encouraging the business owners are willing to give third and fourth chances and don’t judge or stigmatize.” |

| Pierce County, WA launches new mental health court The nation’s newest treatment court launched this week! The Pierce County, Washington Mental Health Court will continue the county’s strong support for treatment courts with a focus on justice-involved individuals with mental health disorders. Judge Kevin A. McCann said, “We know from experience that the members of our community who suffer from mental illness will benefit from this structured path away from criminality. We are reforming our criminal justice system for the better.” |
| Congratulations to the Adams County, Illinois Drug Court on its 119th graduate! Tashia expressed her gratitude to the program saying, “It’s given me a great support system, so that I’m able to lean on people in my life that care about me, that truly care about me.” |

| HEADLINE OF THE WEEK: “Recovery Court promotes hope, healing in community” Read this great piece out of Tennessee here. |
| Share your National Drug Court Month success! NADCP wants to hear from you. Let us know what you are up to during National Drug Court Month and help your program get featured in our weekly roundup. Click here for submissions. |
The post National Drug Court Month Week 1 appeared first on NADCP.org.

Courts everywhere have mandated that secular, evidence-based addiction treatments, like SMART Recovery, must be offered to individuals as alternatives to 12-Step and other faith-based programs, if they so choose. Much of this is largely thanks to the tireless work of individuals like Sarah Levin.
Sarah is founder and principal of Secular Strategies, a firm specializing in defending the separation of church and state, advocating for religious freedom for all, and empowering nonreligious constituencies. A graduate of American University in Washington D.C., Sarah works on behalf of SMART Recovery on state government relations matters, under the direction of David Koss, SMART Recovery’s Director of Government Relations and current Board Member.
Check out this great interview by Luke Frazier, for our new show Insiders+ Access, made possible in part by the generous support of SMART Insiders+ participants.
Sarah Levin is featured in the podcast, Swimming Against the Legislative Tides
Additional information about the New York legislation bill
For more information on how you can join the SMART Insiders+ Program, go to: www.smartrecovery.org/insiders
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @ 800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!

C.C.’s passion and enthusiasm towards his recovery is infectious. He uses the SMART Recovery tools and resources to cope with urges and manage his addiction. C.C. is happy to share his journey with others, in order to help them live Life Beyond Addiction.
Subscribe to the SMART Recovery YouTube Channel
Video storytelling is a powerful tool in recovery, and we are proud to share our SMART Recovery content free-of-charge, available anywhere, on any device. Our videos hope to inform, entertain, and inspire anyone in the recovery community.
Subscribe to our YouTube channel and be notified every time we release a new video.
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @ 800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!
The question of how to describe and categorize addiction has been the subject of several of my recent posts. Some people scratch their heads about why I care so much about whether we think of it as a disease. Bill White summarized the stakes well here:
If AOD problems could be solved by physically unraveling the person-drug relationship, only physicians and nurses trained in the mechanics of detoxification would be needed to address these problems. If AOD problems were simply a symptom of untreated psychiatric illness, more psychiatrists, not addiction counselors would be needed. If these problems were only a reflection of grief, trauma, family disturbance, economic distress, or cultural oppression, we would need psychologists, social workers, vocational counselors, and social activists rather than addiction counselors. Historically, other professions conveyed to the addict that other problems were the source of addiction and their resolution was the pathway to recovery. Addiction counseling was built on the failure of this premise.
White, W. (2004). The historical essence of addiction counseling. Counselor, 5(3), 43-48.
Whether we define alcoholism as a sin, a crime, a disease, a social problem, or a product of economic deprivation determines whether this society assigns that problem to the care of the priest, police officer, doctor, addiction counselor, social worker, urban planner, or community activist. The model chosen will determine the fate of untold numbers of alcoholics and addicts and untold numbers of social institutions and professional careers.
The existence of a “treatment industry” and its “ownership” of the problem of addiction should not be taken for granted. Sweeping shifts in values and changes in the alignment of major social institutions might pass ownership of this problem to another group.
White, W. L. (1998). Slaying the Dragon: The History of Addiction Treatment and Recovery in America, page 338
I’ll acknowledge that hustles like patient brokering, cash MAT clinics, drug screen scams, and over-priced residential with little continuing care make it difficult to root for the survival of the “treatment industry” but White’s words capture the risks of transferring responsibility to other groups.
What’s made addiction counseling unique has been the emphasis on recovery as the endpoint. More specifically, a model of recovery that results in people with addiction becoming “better than well.”
An essential step in transferring responsibility from one group to another is redefining the problem.
Some efforts to define addiction as something other than a disease argue that it’s not a disease but, more often, arguments against the disease model are more about achieving particular goals (protecting liberties, assigning personal responsibility, advancing particular drug policy goals, advancing social justice, emphasizing particular interventions, stigma reduction, etc.) rather than really questioning whether it’s actually a disease.
Recently, the American Journal of Public Health published an article titled The Harms of Constructing Addiction as a Chronic, Relapsing Brain Disease. I appreciated the clarity of its arguments.
The article opens with the following paragraph:
As an international network of historians and social scientists who study approaches to the management of drugs across time and place, we have noticed the effort to redefine addiction as a chronic, relapsing brain disease (CRBD). The CRBD model is promoted as a route to destigmatize addiction and to empower individuals to access treatment that works within that model’s terms.1 CRBD usefully recognizes that brain-based neural adaptations place individual brains in chronic states of readiness to relapse. But brains are housed inside of people. Substance use is biological, social, and political; our concepts and approaches to complex questions surrounding substance use must be, too.2,3 By overlooking the sociopolitical dynamics and inequalities bound up with substance use, the CRBD model can paradoxically further marginalize people who use drugs by positing them as neurobiologically incapable of agency or choice. We are concerned that the CRBD model paints drug users as individuals whose exclusion from social, economic, and political participation is justified by their biological flaws and damaged brains.
Note that the authors respond to an argument for what the disease model can accomplish — it “is promoted as a route to destigmatize addiction and to empower individuals to access treatment” — rather than to the argument that it is properly classified as a disease.
All illnesses occur within people and have biological, social, and political contexts. Over the past couple of years have reinforced that those contexts have important implications, even with something like a respiratory illness caused by a virus. That COVID is associated with social, economic, and political disruption, conflict, and suffering shouldn’t and wouldn’t lead us to questions about whether COVID is properly framed as a disease.
Choosing between the CRBD model and addressing the sociopolitical dynamics and inequalities seems like a false choice. Why does it have to be either/or? Cant it, shouldn’t it, be both/and?
No responsible advocate of the chronic relapsing brain disease (CRBD) model would argue that people with addiction are incapable of agency or choice. Addiction is a disorder involving choice, but it is typically characterized as impaired choice or intermittent loss of choice, rather than a complete or consistent loss of choice. One might compare this to serious mental illness with intermittent fluctuations in impairment. These fluctuations in impairment may range from no impairment to severe impairment, depending on the individual and the current state of their illness.
It’s also important to note the authors’ switch from discussing the CRBD model in the context of people with addiction to people who use substances. The CRBD model should never be applied to people without addiction.
The article proceeds with a brief examination and critique of the CRBD model. The authors note that advocates of the CRBD model voiced hope that the model would produce a sharp break from the moral models that had dominated responses to addiction.
The supposedly new CRBD model recycles disease concepts that have mixed medical and moral concerns since the 18th century.9 Disease models have been used to support a range of policy approaches from strict prohibition, to compulsory treatment or “civil commitment,” to medical maintenance, to incarceration. In them, addiction has been both criminalized and medicalized; addicts were labeled as sick individuals yet also punished for bad behavior as deviants….
Despite the hopes placed on the new CRBD model, this heritage has not been erased by redefining addiction as a chronic disease located in the brain.11 On the contrary, the brutal social inequalities of US responses to drug-related harms have persisted or even worsened.
Note that this is not actually criticism of the CRBD. Rather, it’s criticism of the fact that the CRBD has not delivered the change in policy and attitudes that many people hoped for.
Framing Addiction as a Chronic, Relapsing Brain Disease
It continues with the suggestion that the CRBD may have accelerated these harms in ways that include criminalization, incarceration, and a molecular orientation that opened the door for the opioid crisis with the false belief that Oxycontin’s extended-release formulation might make it safer.
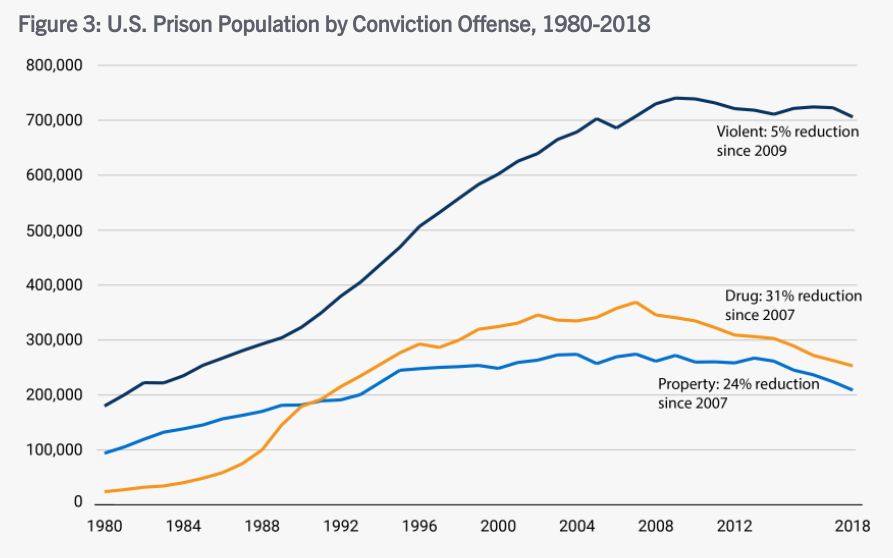
I’m not a believer that the CRBD necessarily leads to less stigma and better policy, and I won’t suggest that the CRBD is responsible for any changes in policy. However, the argument that the CRBD model is associated with incarceration is undermined by trends in incarceration for drug crimes. Even if the CRBD model could deliver significant policy and cultural change, that would take time — years, probably many years. The chart below shows a leveling off and eventual decline of people incarcerated for drug crimes during the period discussed. It’s still too many people incarcerated and those people are disproportionately African American but, if we want to assert an association between the CRBD and incarceration rates, the association would be a downward trend in drug crime incarcerations.
-

A liver cure containing 90% alcohol. -
“mild… statistically insignificant side effects”
The Oxycontin argument would be a lot stronger if there wasn’t a long history of pharmaceutical advertising that misrepresented the safety profile of medications, often misrepresenting science to obscure the risks.
So… the criticism is not about the scientific or medical truth of the model, rather it’s about insufficient political and social progress.
This section ends with a strong point:
Expanding access to addiction medications without inclusive social policies and harm reduction has not been enough to prevent or stem America’s opioid crisis.
Calling something a brain disease does not and should not narrow our attention to pills and procedures. Behavioral, psychological, and social interventions ought to be particularly important with a brain disease, particularly since a brain disease is likely to affect those domains and those domains are largely experienced in the brain.
Alternate Frame: Harm Reduction and Social Justice
The authors offer harm reduction and social justice as an alternative frame:
There are other ways of framing and responding to substance use. The most promising of these is harm reduction, a 50-year-old social movement mounted against repressive drug policies. Rather than centering on the brain and embracing abstinence as a goal, harm reduction prioritizes the health and social inclusion of people who use drugs.
Note that the authors are not really speaking to causes or treatments and there’s no reason the recognition of a condition as a disease should omit social inclusion. For example, serious mental illnesses are recognized as diseases and social inclusion should be considered an essential element of effective treatment and policy.
So, what is the concern?
Consumers resist the coercive and often punitive ways in which medications for addiction have been deployed. Harm reduction links the biological to the social without prioritizing one over the other.
So, a concern is coercion. Calling something a brain disease does not necessitate coercion (think Parkinson’s), but it can open the door. In the medical world, that door might be opened through the legal designation of a guardian. With mental illness, involuntary treatment may be sought for patients that pose a risk to themselves or others. In the cases of guardianship and court-ordered treatment for a mental health crisis, there are processes designed to protect the rights of the individual, including time limitations on any court order resulting from the process.
In the case of addiction, involvement with the criminal justice system often leads to coerced treatment. And, there has been far too little systemic ambivalence about individual rights when it comes to coerced treatment (and incarceration) for addiction. Importantly, there’s also been too little concern about systemic injustices, like the disproportionate numbers of African Americans charged and convicted of drug crimes.
Addiction is also unusual among diseases in an important way. As Keith Humphreys pointed out, “To use a term from economics, addictions have high negative externalities that most medical disorders simply do not, and that changes how perfectly decent and reasonable people respond to them.”
To illuminate those high negative externalities, Humphreys poses the following questions:
If you had a financial manager who would have access to all your accounts and personal information, would you consider that person developing a heroin addiction of any more consequence than him/her developing type 2 diabetes? If you were enrolling your child in a preschool, would you react in the same way if informed that the teacher was prone to methamphetamine binges as you would to learning that the teacher was prone to asthma attacks? If asked by a non-expert from outside our field, how would you explain why millions of people have chosen to attend self-help groups and treatment programs focused on recovering from having had an ‘‘alcoholic’’ parent, but there is no demand for recovery programs focused on adult children of hypertensive patients?
Acknowledging that there has been insufficient concern for individual rights, I suppose at least 4 considerations are important regarding coerced treatment.
- Do the circumstances merit limiting the liberties of the person (through court supervision, incarceration, or coerced treatment)? Is this a circumstance where others were harmed or at serious risk of harm? If we removed the substance from the situation, would this still be a matter for the criminal justice (or child protection) system?
- Treatment for what? What is the person’s substance use problem and is the treatment appropriate for that problem? Are we talking about someone with a mild, moderate, or severe problem? Are we talking about someone with a pattern of impaired control?
- Coerced treatment is often an alternative to incarceration. This is a good thing. However, we should be mindful that this option doesn’t lower the bar for limiting the rights of a person.
- What systemic factors are likely to influence who ends up in this system and how their case is handled? Are we acknowledging and addressing those? If forces external to this system are a problem, how can that be mitigated within this system?
I’m ambivalent about the development of processes for addiction that would mirror the mental health processes. Having worked in both systems, I know it would require a lot of work to protect the rights of people with addiction and an enormous amount of work to develop systems of care that can meet the need effectively.
As for the role of the CRBD model in this area, I do see the risk and I do sometimes hear the CRBD model deployed to defend coerced treatment. At the same time, the period of time the authors point to has been characterized by efforts to reduce incarceration and offer treatment as an alternative — on the grounds that addiction is an illness.
I think the CRBD model offers a valuable test for public policy — parity. Would we, should we, treat a cardiac or diabetes patient this way? The high negative externalities identified by Humpreys do present a challenge for parity tests using other chronic diseases, but he offers another frame. He’s talking about it in the context of public education, but it’s relevant for thinking about policy as well.
A better analogy than asthma, type II diabetes, and hypertension we could employ for addiction might be to liken it to chronic infectious illnesses (eg, HIV/AIDS). We accept that for infectious illnesses, some fear of people who have the disease is rational; indeed health professionals exhort people to engage in behavior designed to protect themselves from infected individuals (eg, insisting that a sexual partner with a sexually transmitted disease wear a condom, not personally cleaning the body of someone who died from Ebola). Further, we accept that there is a legitimate role for law enforcement— Typhoid Mary was prevented from continuing to infect people by police (Marinelli et al., 2013), not doctors. Analogizing addictions to infectious diseases has all the virtues of analogizing it to diseases with low externalities (eg, asthma) and also has the unique advantage of better matching the public’s experience of the disorder (and it is them and not ourselves whom we need to persuade).
Of course, this imagery will evoke strong negative reactions from many, but it also provides the potential to narrow the focus for coercive interventions to those where there is actual harm or serious risk to others.
Uneven Progress: Harm Reduction in Europe
Next, the authors provide a little background on harm reduction in Europe that they summarize as follows:
Harm reduction initiatives across Europe and the United Kingdom were introduced as part of publicly funded institutions that often coexist with repressive drug policy systems—something shown with unusual starkness in the French example. The UK example indicates how harm reduction measures do not always center on social justice for people who use drugs but are instead introduced to protect the majority population. The Norwegian example points toward how restrictive access to harm reduction services can facilitate paternalism and reduce agency of people who use drugs.
Conclusion: Human Rights as an Expanded Harm Reduction Frame
…The human rights frame counters some of the CRBD model’s limitations, including the centering on brain disease pathology and insistence on judging each individual as either a patient or a criminal.
People who use drugs are themselves developing community-based harm reduction approaches that resist both criminalization and medicalization on the ground that both have been used to control drug users. Harm reduction critiques hierarchical forms of clinical and neuroscientific expertise and instead supports people who use drugs in recognizing their expertise in managing their own practices and bodies, supporting their agency, and widening their options. Abstinence can be considered part of this approach, but only if chosen by people who use drugs themselves.31 When abstinence is imposed by external forces (medical practitioners, family, law enforcement, or other stakeholders), abstinence itself becomes a risk for overdose death.
This illuminates another objection, that the disease label situates the person with addiction as a patient. (As opposed to a criminal.) It’s also important to note that the authors switched from addiction to “people who use drugs.” This switch is important because using drugs isn’t a disease but may be a symptom of the disease of addiction, just as coughing isn’t tuberculosis. To be sure, most people who use drugs do not have the disease of addiction. Differentiating between people with addiction and other people who use drugs is critically important in many ways, but particularly important when discussing the disease model, its conceptual boundaries, and its utility.
The framework of disease is helpful because it helps us draw a boundary to determine who has the disease and who does not, it can help us understand some of the processes involved and their consequences, it can help us identify treatments, and help us identify treatments, behaviors, and interventions that are contraindicated.
The authors seem to be very focused on protecting the right to choose to use drugs. For the minority of users with addiction, a critical element to understand is impaired control, meaning that drug use is not always freely chosen. (One might even say that, at times, the illness coerces the sufferer to use drugs. This is part of what’s so excruciating for people with addiction and their loved ones.) This is one of the reasons that, for this most severe form of drug problems affecting a minority of users, abstinence is indicated.
People with bipolar or schizophrenia have the right to refuse treatment in most circumstances. However, when their illness results in high negative externalities, they may be coerced into treatment via a process that includes several safeguards to protect their liberties.
So… this critique never seems to make a case that addiction is not a disease. Rather, it argues that the CRBD model has not delivered the change some people promised and they proposed a model centered on the social and political change. I don’t see where an emphasis on social justice requires the abandonment of the disease model. In fact, where high negative externalities are present, the disease model becomes a mitigating consideration, resulting in more just social responses.
I believe it’s true that addiction is a disease and the authors never really made an argument that it isn’t. Should that truth be sacrificed or obscured in pursuit of justice? I don’t think it’s a good idea. It’s the kind of thing that contributes to the current epistemic crisis and it isn’t necessary. Any model can be harmful if it’s misused or implemented in a reductive way that results in the neglect of important considerations. The CRBD is no different.
You can’t put a dollar value on the losses American families have suffered due to the addiction and overdose crisis. A life lost to overdose is irreplaceable, and the costs to happiness, success, and well-being of those living with addiction are similarly overwhelming and incalculable. Yet, funds are finite, and public health decisions do carry cost implications. When policymakers and community leaders can translate the human benefits of effective treatment and prevention measures into some quantifiable return on that investment, it can be a lever to shift public health policies.
Recently in the journal Prevention Science, a group of researchers funded by the National Institute on Drug Abuse (NIDA) published an analysis of the costs to North Carolina healthcare payers for hospital charges potentially relating to higher-risk behaviors in patients aged 9-18 (i.e., pre-adolescents and adolescents) in 2012. Charges included care for injuries from violence, accidents, or poisoning; care relating to sexual activity, substance use, or psychiatric disorders; and charges related to suicide or self-inflicted injury.
The researchers found that these charges totaled more than $327 million, accounting for more than 10 percent of all hospital-related charges. The higher-risk behaviors associated with these costs are preventable with psychosocial interventions, including family-based prevention programs. Pediatricians and family therapists surveyed in the study supported screening and referral to prevention, but cited possible challenges to reimbursement for these services as well as lack of training and lack of referral networks to/from each other. Pediatricians also cited concerns over patients not following through with referrals, suggesting that having family therapists working in pediatric clinics could help.
Primary prevention—including screening and intervention before negative health outcomes occur—is relatively inexpensive, and the higher-risk behaviors it is designed to reduce are so costly to the healthcare system that it is staggeringly wasteful not to make sure that screening and treatment referral are readily implemented and faithfully reimbursed by insurers and that interventions are convenient for parents and their children.
Reducing higher-risk behaviors would lessen burden across many sectors of society, not just healthcare, which was the sole focus of the newly published analysis. Greater investment in preventing such behaviors in youth would yield savings across public safety and the criminal justice system, behavioral health, education, and so on.
This is a common theme in the research on the benefits and costs of prevention. Some programs designed to prevent teen substance use and other behavioral problems have been found or estimated to be stunningly good investments. For example, an early childhood intervention called Nurse Family Partnership, in which specially trained nurses periodically visit first-time mothers during their pregnancy and first two years of their child’s life, was shown in an analysis by the Washington State Institute for Public Policy to save taxpayers $2.88 for each dollar invested; the same analysis found that a component of an elementary-school-based intervention called the Good Behavior Game saved taxpayers $25.92 for each dollar.
Another example is the Communities That Care prevention system, developed three decades ago and the subject of many randomized trials that follow participants well into adulthood. Communities That Care is not a single prevention intervention but a structured approach that helps communities utilize their resources most effectively to address identified risk factors for substance use, aggression, and other problems in youth. One recent analysis showed that an approximately $602 investment in each child (adjusted to 2017 dollars) had yielded an estimated $7754 in savings by the time participants were age 23—a $12.88 return for each dollar invested. The researchers estimated that those savings were distributed among individuals/families themselves, taxpayers, and other stakeholders. The return was well over twice as great when the downstream economic benefits of completing college—more likely among those receiving interventions—was factored in.
Prevention is needed now more than ever. Fentanyl is permeating the illicit drug supply and causing ever-greater numbers of overdose deaths. It is increasingly found in counterfeit prescription pills, which are liable to be taken by youth and other people with no previous exposure to opioids. In 2020, for the first time, fentanyl overdose deaths in teens spiked to nearly double the rate it had been in previous years.
Communities, schools, and healthcare systems already have scientifically well-supported tools at their disposal to help prevent substance use and other related mental illnesses and risk behaviors in adolescence, but sadly they are seldom implemented. Even if an intervention can be shown in a trial to produce benefits, it cannot be expected to make a positive impact if it is not easily scaled up in a variety of real-world settings adaptable to the needs of different communities. For this reason, developing and testing interventions that can be adopted and sustained is an important part of NIDA’s prevention research portfolio.
While investment in prevention doesn’t show immediate returns, playing the long game and investing in prevention interventions can save lives and dollars.

An interesting discussion with a passionate advocate for MAT expansion and the most prominent advocate for the “new paradigm“:
What is the process for successfully integrating these 2 approaches? What are the biggest hurdles providers face when accomplishing this goal?
Dr DuPont: The biggest hurdle is the staff reluctance, even the staff distaste, for the integration of an alternative as an option for patients who want it. There is an ideological and visceral rejection of the integration at the start that is challenging. But with gentle persistence, it has been overcome and the patients have benefited.
Dr Poland: I also find that patients are a bit reluctant to share their experiences with 12-Step—good or bad—somehow, they’re expecting a reaction from me—either insistence they go or disdain for the program. Again, being open and nonjudgmental about what works for an individual allows us to best care for them. And, I’ve definitely learned a lot from my patients about how to integrate the 2 modalities in a way that complements each other.
I’m looking for a recording.
As substance-free definitions of recovery are challenged, this article on Stanford’s substance-free student housing community made me wonder if some recovering students will find more safety and support, and have more in common with fellow students in these communities than in collegiate recovery programs (CRP) that include students whose definition of recovery includes ongoing substance use.
Maybe this kind of housing option gives a CRP more space to stretch their boundaries, knowing that there is a substance-free peer group elsewhere on campus? Maybe it offers a path to support these students and sidestep culture wars about the definition of recovery? IDK, and I know nothing about those dynamics at Stanford. It just caught my attention and got me thinking. (More here.)
When you’re in recovery, your old methods of relieving stress – having a drink or using a drug – can no longer be utilized. It’s time to build new, healthier habits that allow you to relax and enjoy yourself while also improving your lifestyle and setting yourself up for future success in your recovery. Below are some tips for healthy stress relief that may seem like common sense, but are oven overlooked and undervalued.
- Do physical activities you actually enjoy. Fitness journeys look different for everyone – but most people will agree that exercise is a great stress reliever. That doesn’t mean you have to go overboard on the treadmill or lift weights at the crack of dawn. Find a routine that works for you, and you’ll be much more likely to stick with it and genuinely enjoy it. When you’re engaged in physical activity, your brain releases endorphins that make you happier. Exercises done daily such as yoga, aerobics, and even simply walking can go a long way towards making you feel better about yourself and your life.

- Maintain a healthy diet. Along with a good exercise regimen, a healthy change in diet will help prevent negative feelings and regret that accompany a junk-food binge. Again, this doesn’t mean you have to go overboard – take small steps to create a greater lifestyle change that you’re more likely to keep up with. When you eat healthier, your mood improves
- Build better sleep habits. “Eight hours a night” isn’t just something your parents made up – science shows that we are more productive, have better memory, and are overall happier when we fit enough sleep into our schedule. Running on less sleep leaves us ill-equipped to handle life’s challenges, which inevitably leads to a buildup of stress.
- Talk it out. Opening up certainly isn’t an easy task, especially for those in recovery who are used to isolating and self-medicating rather than speaking their mind when they’re struggling. In treatment, you discover how important and necessary talking about your feelings can be – don’t lose that ability once you’re in the real world. Continue having discussions with your loved ones and your recovery support network. Don’t keep anything bottled up. Your stress levels will drastically decrease as you get things off your chest and receive verbal support and feedback from those around you.
Remember that being kind to your body, no matter which way you go about it, is the best way to relieve yourself of stress, whether internal or external. When you practice healthy ways of coping with stress, you’re reinforcing those behaviors in ways that make you more likely to keep up with them, though they may seem difficult or tedious at first. As in recovery, stress relief is a constant battle that must be taken seriously and dealt with in healthy ways.
For more information, resources, and encouragement, “like” the Fellowship Hall Facebook page and follow us on Instagram at @FellowshipHallNC.
About Fellowship Hall
For 50 years, Fellowship Hall has been saving lives. We are a 99-bed, private, not-for-profit alcohol and drug treatment center located on 120 tranquil acres in Greensboro, N.C. We provide treatment and evidence-based programs built upon the Twelve-Step model of recovery. We have been accredited by The Joint Commission since 1974 as a specialty hospital and are a member of the National Association of Addiction Treatment Providers. We are committed to providing exceptional, compassionate care to every individual we serve.