[Ed. Note: big thanks to SMART Volunteer Anne Devenport for writing this guest blog]
The DISARM tool is used in SMART Recovery to deal with urges – participants in recovery meetings imagine that an unpleasant salesperson is trying to push them into their addictive behavior, so they use the DISARM tool (Destructive Imagery and Self-Talk Awareness Method) to help them deal with the imaginary salesperson, and so deal with their urges.
A participant once asked during a Family and Friends meeting if it would be possible to make the DISARM tool relevant for Family and Friends. We might first start by identifying what the salesperson might be tempting us, as Family and Friends, to do.
We might feel strong urges to:
Nag our Loved One
Protect our Loved One
Clean up our Loved One’s messes
Call our Loved One’s boss to explain why they are late
Hide our Loved One’s behavior from others
Give our Loved One money for their addictive behavior
Fix our Loved One’s problems
….. and many other things
The DISARM tool suggests that we might call our salesperson a name (The Creep, The Sleazeball), and that we might tell the salesperson to get lost. In this way we are personifying our urge to fix/protect/nag, which might help us to recognize that the urge isn’t part of us, and that we have the power to refuse it – to refuse the salesperson.
There are a few questions we might ask ourselves when the salesperson turns up in our lives. Let’s examine the DISARM tool from the point of view of someone who wants to jump in and fix their Loved One’s problems – they want to buy them a new cell phone when their Loved One has broken theirs; they want to repair their Loved One’s fender bender; or they want to vigorously edit their college-aged son’s homework to prevent them from getting a bad grade. The questions of DISARM for Family and Friends might look like this:
Do I have to fix my Loved One’s problems just because I strongly want to?
Our answer might be:
“No, it would be easy to give in, but I don’t have to. I have resisted
fixing in the past, despite the demands of the salesperson, so I
know that I can do it.”
Will it be awful to stop myself from fixing my Loved One’s problems?
Here we might tell ourselves:
“No, it won’t be awful. It might be unpleasant to watch my Loved
One trying to fix their own problems, but it won’t be awful. If I
don’t give in to the salesperson this time, it will be easier to resist
in the future. I know that in the long-term my stepping back from
fixing everything might be helpful for my Loved One – it will send
them the message that I have confidence that they are capable of
fixing their own problems.”
Am I somehow entitled to have an easy life when dealing with my Loved One?
We might answer this with:
“No, I am not entitled to an easy life with my Loved One. The
salesperson is going to keep on trying to tempt me, that’s just a
fact of life, and I can deal with it. Like everyone else, I encounter
difficulties in life, and I know that I can work through these.”
Additionally, whenever the salesperson rears their unwelcome head, and tempts us to jump in to fix our Loved One’s problems we can turn to section 10 of the Family and Friends Handbook, where we find the following questions:
Will changing my behaviors truly hurt my Loved One? Yes, they may get angry, but what is that in comparison to the long-term harm of addiction that I am working to avoid?
What will hurt me more: changing my behaviors, or knowing that I didn’t do anything to change my behaviors?
What can I expect to happen if I don’t change? Will things get better?
So, at the risk of sounding like a salesperson…consider buying into DISARM – another great SMART tool that we can add to the Family and Friends toolbox.
Working in the substance use service system has always been a challenge. This was true even from its early days. We help people in some of their most difficult moments with few resources to support what they need to get well. We operate under constant triage conditions. Yet despite this, we tend to oversell those shining moments of reward experienced helping a person on their recovery journey to get people interested in taking on the calling of serving people in our SUD care system workforce. Maybe we should instead tell recruitment prospects the truth.
Many of us love this work. We can play a part in people saving their own lives and redefining how they want to live. We witness the immense changes that can occur in ways that change the trajectory of whole families and at times large swaths of the community. Lives are changed in part because of the work we do. This is also essentially our workforce recruitment narrative.
It will be obvious to most that I lifted part of the title of this post from the US Marine Corps. It may seem overly dramatic, but there are parallels at least in one way. The Marines go to where they are needed, when they are needed, whether or not they have the resources to do the job. This is not an uncommon experience in the SUD service environment, particularly in the public sector. We serve because we are needed, often without the things we need to do the job because lives hang in the balance. Triage and improvision are the tools we far too often have to do our jobs. That is the truth for so many of us.
Despite this, we lead with the warm fuzzy good stuff despite the cold hard reality of the work. Perhaps it is not the right way to recruit people for our field. I have come to this conclusion following a lot of conversations with people in diverse settings across our system in recent weeks with a lot of common notes and themes. We need to tell the truth about the work to those who are considering a career in our field. Failure to do so is a set up as fresh-faced workers once they experience what it is really like in the trenches. Vital work that tests your skills and stamina.
Far too often in this era, our workforce is dealing with death in a close up and intimate way, perhaps in no greater frequency than within our peer workforce. In the age of Fentanyl and Xylazine, care is more complicated, recovery efforts more challenging and the risk of lethality dramatically increased. I was unable to find much in respect to SUD treatment protocols or recovery engagement strategies beyond withdrawal management for this new trend. Front line workers with direct experience have shared with me that persons using these drugs together are more challenging to engage in a change process. This is also historically the case as academic data lags practice as new drug use patterns unfold. But in this I am hopeful.
I know that history shows us that it is these same front-line workers who will find practice strategies that will help improve outcomes over time. Every prior emergent drug use patten has shown us that it is our frontline workforce who figure things out in ways not unsimilar to how Mobile Army Surgical Hospital workers learn to improvise in the moment and adapt to save lives. Grim, challenging, and imperative work that does not translate well to a feel-good recruitment campaign. Such work is not for everyone.
The work takes a toll on you. You see and experience traumatic things that will stay with you for the rest of your life. Resumption of use can be a risk, as can be experiencing high levels of stress, secondary trauma and even potentially the risk of physical harm. All far too often for less money and longer hours than slinging burgers.
It is a space ripe with snake oil sellers, hustlers and hucksters. Also not a new trend, they have been around well before the era of the “Keeley Cure” which included gold injections to cure alcoholism that became popular a millennia ago. All the resources to address our current crisis have brought out a host of these kinds of people promising solutions marketed in the most appealing ways. They often find their way to the front of the line because they offer compelling and simple solutions to situations that in truth defy such simplicity. It can take awhile to play out as they burn through resources. All of which can be quite disillusioning for people seeking to do this work for better reasons than to make a lot of money or to become a guru. We need recovery custodians dedicated to hard work, not rockstars who burn bright and far too often leave us with more devastation and fewer resources when the inevitably implode.
Other long-term challenges in our field are being exacerbated by our current circumstances. High quality, consistent supervision has always been a challenge perhaps in no small part to the triage dynamic of the work. Supervision while under fire often seems secondary even as it is critical. Supervision is getting even harder to find due to the increasing loss of experienced workers. Experienced workers are retiring, giving up on the work due to the mountains of paperwork and incessant bureaucracy or simply taking jobs that pay more, which includes most other types of work without regard to training, educational level, or experience. Often for more pay, fewer work hours and lower stress. I cannot recall a conversation with seasoned colleagues in the last year that did not include the myriad of reasons to just do something else, yet many of them carry on. Yet attrition is occurring, which leaves fewer mentors for less experienced workers who far too often are learning through trial and error.
It is important to understand that most everything in this piece was true 20 years ago but we kicked the ball forward. Over the decades policymakers struggle to prioritize needs without the capacity to meet the ones on the table. They have been constantly challenged with triaging the crisis of the moment with limited resources to address anything not on fire. Workforce development has consistently seemed to be the thing we will address tomorrow when the current crisis ends. There is always a new crisis.
Because of all of these dynamics, it is also true that recovery far too often occurs despite our care system and not because of it. Our systems have long been designed to deliver band aids instead of habilitation and long term support. We provide comfort care or short-term treatment in ways that deliver people back to our front doors or an early grave and not long-term recovery, which remains not much more than an afterthought. Our workers far too often find themselves working in systems of care that don’t work. Helping people heal in these kinds of environments takes a lot of courage, stamina and can at times feel like an act of defiance.
Pointing out these truths in our systems can be dangerous. Far too often truths are uncomfortable, and a lot of energy can be consumed across our systems of care avoiding them. Newcomers to our system often learn this the hard way. They point some things out that become evident to them doing the work on the ground and get swatted down by the system. This is perhaps no truer than for recovering people with the asset of lived experience being eclipsed and discounted due to the deep sense of unworthiness and distrust our society has for people who have experienced addiction so pervasive in our healthcare systems and beyond. There is also an inverse relationship between resources and proximity to the problem. The closer to the street you are the less resources and credibility you have, while the money and answer people are far removed from the reality of real-world conditions. This too is because of stigma.
So when all else fails, perhaps we should tell the truth. It is not a job; it is a calling, and not an easy one. We do this work because it is vital, not because it is easy or that everyone we work with has a fairy tale outcome. We are simply not working in that kind of environment, and even properly resourced the gravity of the work is life and death, not the thing of fairy tale endings, at least our modern versions of them. Despite it being hard and far too often done in the face of stiff headwinds and a sea anchor fastened to our stern, we push forward. We do so because we must.
The final irony is that when our efforts fall short because we are under resourced and meager resources are rationed out like thin gruel, it gets played as the clients are failing or our workforce is failing and not that we were never resourced to succeed but instead to triage. This is true for any highly stigmatized condition, but perhaps none more so than ours.
If we tell the truth about how difficult it really is, perhaps it will draw people in who are more intentional about why they want to serve our communities in need. And perhaps with such truth telling we may actually end up helping us address these systemic challenges in ways that things actually do change.
To those of you out there who get up and do the work knowing the above truths and do it anyway. I salute you.
And for those who think you can navigate all the above, the hardest job you will ever love, we welcome you. We need you!
Dr. William Miller
The 2023 Richard Saitz Memorial Lecture registration is now open! We are pleased to welcome Dr. William Miller to present, “Going Upstream: Addiction Care for the Masses.”
Description: Although the vast majority of people with diagnosable substance use disorders will never receive specialist addiction treatment, most will recover. Dr. Saitz was passionate about serving this at-risk population. Drawing on his 50 years of research, Dr. Miller will discuss various ways of “going upstream” to intercede at earlier stages of problem development including (1) teaching moderation skills, (2) brief opportunistic interventions such as SBIRT, (3) motivational interviewing and a person-centered clinical style, and (4) providing behavioral health services within mainstream healthcare.
Dr. William R. Miller is Emeritus Distinguished Professor of Psychology and Psychiatry at the University of New Mexico having served as Director of Clinical Training and as a Founder and Co-Director of the Center on Alcoholism, Substance Abuse and Addictions (CASAA). His publications include 65 books and over 400 articles and chapters. Fundamentally interested in the psychology of change, he introduced the method of motivational interviewing in 1983. The Institute for Scientific Information has listed him among the world’s most cited scientists.
Richard Saitz, MD, MPH was a leader in the addiction treatment world and a friend of SMART Recovery. He was a keynote speaker at our 25th Anniversary Conference in 2019. You can read more about Dr. Saitz’s life and accomplishments here
In a recent post, I tried to unpack “drug policy” to look beyond legal/illegal and think through the kinds of things that drug policies determine and influence.
Historically, it seems that concerns about the harms associated with drugs have overshadowed the harm associated with policies that seek to prevent those harms.
It seems particularly important at this time to acknowledge the direct and indirect harms associated with drugs, and the direct and indirect harms associated with drug policies.
Several articles published within the last couple of weeks brought that post and the role of policy to mind.
Addicted to Cannabis?
The NY Times recently published an article on cannabis use and addiction. It raises questions about trends in use (also addressed in this recent article), the relationship between those trends its legal status, how differences in harms influence the ways drugs are thought about, and how problems are conceptualized by the public, journalists (the authors equate cannabis use disorder and addiction), and professionals.
Julian (who asked not to use his last name when talking about a sensitive medical condition) didn’t have much of a social life, so he started smoking by himself to pass the time. “Weed became my friend,” he said. “I would get off work and I would smoke because I was bored.”
Soon, Julian’s life began to revolve around cannabis. Smoking never interfered with his work, but it stopped him from doing just about everything else. “Typically, when you move to a new city, you establish new relationships, and I was doing none of that,” he said. “I was living almost like a recluse.”
…Despite the common misconception, people can become addicted to cannabis just as they can with other drugs, like alcohol or cocaine. As more states either decriminalize or legalize cannabis, more people are using it than ever before. According to the National Survey on Drug Use and Health, in 2021, approximately 19 percent of Americans 12 and older used cannabis, and nearly 6 percent of teens and adults qualified as having cannabis use disorder…
…The potential consequences of cannabis use disorder are not as severe as with other drugs like opiates, where overdose deaths are a dire concern. But cannabis addiction can cause “a dramatic decrease in quality of life,” said Dr. Christina Brezing, an assistant professor of psychiatry at Columbia University.
This Bridge Michigan story raises questions about policy influences price, how price influences use patterns, industry consolidation, and the creation of adjacent business sectors.
…as revenues rose for recreational use, the price of marijuana has plummeted. The average price of an ounce of recreational marijuana was $160.10 in February of last year compared with $86.00 this February.
Experts say one reason the price for marijuana is constantly decreasing is to encourage more consumers to buy it legally, rather than from illegal sellers.
“Even though prices are falling, there’s more people buying in the legal market [and] that’s what’s driving the increase in overall revenue,” said Beau Whitney chief economist for the National Cannabis Industry Association.
An oversupply
Others say oversupply is driving down the price of marijuana.
The Michigan cannabis industry started to become oversaturated with products about a year ago, causing prices to decrease, said Corbin Yaldoo, founder of Corbin Ventures, a commercial real estate development and investment firm in Bloomfield Hills that specializes in cannabis real estate.
“The larger operators have more capability of selling products at a cheaper price,” he said. Because larger operators are able to do this without taking a loss, they ultimately have control over the market.
“Michigan is in its consolidation stage right now, so larger operators are acquiring smaller operators or they’re merging together,” he said.
There isn’t anything that can be done immediately to help suffering businesses, but Yaldoo said lawmakers should limit how much cultivation space they allow growers.
The state currently has 753 active licenses for class c marijuana growers, who can possess up to 1,500 plants according to state law.
Changes in Alcohol Consumption Sharpen Health Inequalities
A recent Lancet article describes the consequences of changes in alcohol consumption patterns, the role the alcohol industry plays in the dominant public health narratives, and how those narratives obscure the inequities associated with those changes in consumption.
Alcohol-specific deaths (encompassing those deaths that are a direct consequence of alcohol, such as alcohol-related liver disease) in the UK have taken an extremely concerning turn, with the Office for National Statistics reporting 9641 such deaths in 2021—the highest on record and a 27·4% increase since 2019 (n=7565).1 This number of deaths reflects alcohol consumption trends since the pandemic, during which drinking patterns became more polarised, with people who were drinking lower amounts before the pandemic on average, drinking less, and people who were drinking higher amounts before the pandemic drinking more.2 This change represents a substantial sharpening of health inequalities, driven by changing consumption patterns of a harmful product.
Communications from the UK’s alcohol industry via their responsibility body, the Portman Group, present a different situation. In 2022, communications from the Portman Group published infographics that drew attention to declines in overall average alcohol consumption, emphasising that “the majority of UK drinkers consume alcohol responsibly”.3 The industry also explicitly links its activities to declines in average alcohol consumption. In an evidence submission to the Scottish government on minimum unit pricing,4 the Portman Group stated that it, along with others, has “played a role in supporting these falls in consumption and harm”, citing corporate social responsibility initiatives like the UK Responsibility Deal (which an independent evaluation found to not be effective5), funding DrinkAware (which independent research has shown communicates misinformation on alcohol-related harms6); and supporting community alcohol partnerships (for which there is little evidence of effectiveness).
The responsible drinking language used in these statements has been found to be overwhelmingly used by industry, rather than other stakeholders like government health departments or independent alcohol charities.8 Such language has been described9 as strategically ambiguous, designed to build positive impressions of an industry that appears to foster responsible use of its product, but with little evidence of effectiveness for responsible drinking campaigns. Crucially, talk of a responsible majority implies that people who drink large amounts of alcohol are somehow irresponsible, and that it is their apparent susceptibility which is to blame. This framing also implies that alcohol harm is a problem only for people drinking the most amount of alcohol, whereas the evidence is clear that alcohol causes substantial harm beyond this group.10
Across 32 months of implementation, we found a significant 13% reduction in deaths wholly attributable to alcohol consumption compared with our best estimate of what would have been expected had the legislation not been implemented. This is equivalent to avoiding 156 deaths per year, on average. There was a corresponding estimated reduction of 4% in hospitalisations for conditions wholly attributable to alcohol consumption, equivalent to avoiding 411 hospitalisations per year, on average. The use of a controlled interrupted time series study design allowed us to infer that the estimated impacts were plausible causal effects attributable to MUP legislation.
Exploratory analyses indicated that the largest reductions were estimated in the 40% most socioeconomically deprived areas in Scotland, indicating that the implementation of MUP has had a positive impact in tackling deprivation-based health inequalities in alcohol health harms. The implementation of MUP legislation was associated with reductions in deaths wholly attributable to alcohol consumption for males and females. Furthermore, we found associated reductions in the age groups of 35–64 years and 65 years and older, but were unable to evaluate change in the 16–34 years age group due to the relatively small number of deaths for this group. The positive impact of MUP legislation by population subgroup was generally similar for hospitalisations, although to a lesser degree.
In this study, we assessed effects of outlet densities on six alcohol-related crimes during weekday, weeknight, weekend day and weekend night hours… we measured relationships between crime outcomes and outlet densities for different days and times. Strong evidence supported differences in DUI, assaults and robberies by day and time. DUIs and assaults occurred more often in areas with more bars or pubs on weekend nights. …Moderate evidence supported differences in IPV (interpersonal violence) by day and time.
This snippet from an email newsletter from the Detroit News raised questions about the influence of drug industries on public policy only tangentially related to drugs.
If you were going to the polls on this morning 110 years ago, you saw this in your Detroit News:
In the April 7, 1913 Detroit News, a short piece describes who can vote in that day’s election, in which women’s suffrage was on the ballot.
Women were voting, too, but only if they owned or shared property with their husbands. On April 7, 1913, full women’s suffrage was on the statewide ballot − and Michigan voters rejected it. (Influenced by a liquor lobby that feared Prohibition would follow, a reminder of the perpetual influence of money in politics.)
Drug policies shape the influence that drug manufacturers and purveyors have. Are they permitted to lobby? Are there any restrictions on their donations? Does tax revenue associated with their industry create incentives to protect them?
Too Few Options for Families Dealing with Addiction
…substance use disorders, if untreated, can lead to criminal behavior, debilitation and — all too often — death. The number of overdose deaths in the United States is higher than ever.
Ideally, people with addiction would seek care. But waiting for a person to choose treatment for a disease that affects rational thought can be catastrophic, now more than ever.
The writer goes on to discuss the policies and interventions that would help, he points to some gaps that make it difficult for patients and families to find and access quality treatment, and the absence of involuntary treatment processes to protect loved ones at high risk for death due to their addiction.
Updates
A couple more papers just came to my attention.
Alcohol Use Disorder Stigma and Responsibility
This Addiction article concludes that alcohol problems are more stigmatized than other mental health problems. This appears to be related to the perceived risk they pose to others and the responsibility ascribed to them.
This fits nicely with some of the references above. The study on alcohol outlet density demonstrates that there are real negative externalities associated with alcohol consumption, and the paper on changes in alcohol consumption patterns speaks to the influence of industry public education efforts emphasizing responsible consumption frame alcohol problems as a failure of personal responsibility.
Our systematic literature search identified 24 publications since 2010, analyzing aspects of stigma toward people with AUD and other mental disorders. The synthesis of findings revealed that stigmatizing beliefs and behaviors toward people with AUD were pervasive in the general population and usually more pronounced than toward persons with depression or schizophrenia. More specifically, people with AUD tend to be perceived as more dangerous and more responsible for their condition, as well as being faced with a greater desire for social distance and a higher degree of acceptance of structural discrimination than people with substance-unrelated disorders.
This Addiction paper looks at the prevalence of alcohol-related harms to others and their distribution among various groups.
Almost half (48.1%) of respondents in this Australia-wide survey reported experiencing one or more harms from others’ drinking in the last year, with 7.5% reporting that they had been negatively affected“a lot” by others’ drinking, and another 26.8% reporting they had been harmed “a little”. Analysing the likelihood of any harm from others’ drinking (including specific harms from known drinkers’ or strangers’ drinking), women, young people, Australian-born (vs. participants born in non-English-speaking countries) and occasionally reported HED (heavy episodic drinking) were more likely to report AHTO (alcohol’s harm to others).Women were more likely than men to be negatively affected both by the drinking of people they lived with and were related to, as well as by the drinking of strangers. In line with previous research, women and young people were at greater risk of AHTO.
More women than men have reported a range of harms from others’ drinking, including arms from intimate partners (24) and financial harm (26) from others’ drinking. This is consistent with previous findings from many countries, including the previous Australian survey (3, 27, 28). Young people are the group of adults that have consistently reported more harms from strangers’ drinking and from drinking of their friends and co-workers (3, 4, 27, 29). In our study, harm from strangers’ drinking was considerably lower for those aged 65 or more than for younger participants, and significantly higher for women aged 18-34 than for middle-aged women. Results in our study are broadly consistent with findings in previous studies that young people report more harms than older adults from strangers’ drinking and from drinking of their friends and co-workers(3, 4, 27, 29).
…women reported substantially more harm than men, particularly from people they knew but also from strangers. This suggests that attention needs tobe paid to reducing harm particularly to women (and particularly younger women) from others’ drinking. Data focusing on differences by this and other social inequalities can provide guidance and benchmarking for policy discussions and interventions.
This article originally appeared in the Milken Institute’s Power of Ideas series.
Our country remains in the grips of an opioid crisis claiming more than 100,000 lives every year. Rising mortality associated with drug addiction and excessive drinking is among the major factors contributing to declining life expectancy. And sadly, the treatments that exist—including medications, in the case of opioid- and alcohol-use disorders—help only a fraction of those who could benefit from them.
The need for new treatments is real and urgent. One aspect of hope amid the tragedy is that the crisis has spurred unprecedented resources and human ingenuity toward finding novel scientific solutions that may one day make addiction a thing of the past.
In the field of substance use and addiction, we have been careful to talk about the management of substance use disorders and the often-difficult road to recovery. Still, we seldom talk about curing these disorders. But recent discoveries and innovations are pointing to astonishing new possibilities for directly intervening in brain circuitry involved in addiction that, if realized, might amount to something like a cure.
Hereʼs an example. A year ago, a multinational team published a landmark analysis of people who smoked cigarettes and experienced damage to various parts of their brain as a result of strokes. Individuals with lesions in areas that had in common a specific pattern of connectivity to a region called the insula stopped smoking altogether after their stroke. This study helped delineate key nodes in the brain that were associated with remission from nicotine addiction. These nodes were also associated with reduced risk of alcohol addiction.
Technologies known as neuromodulation now enable us to alter activity in these and other brain areas without harming them. Transcranial magnetic stimulation (TMS), in which magnetic fields are applied to the scalp to affect activity in the cortex, is already FDA-approved for the treatment of major depression and migraine pain, and the FDA has cleared TMS devices for obsessive-compulsive disorder and smoking cessation.
TMS cannot reach some of the limbic areas (like the nucleus accumbens) that are implicated in addictive disorders, but another method called deep brain stimulation (DBS), which uses electrodes placed in more remote brain areas to deliver electrical current, can. Clinical trials are now ongoing or recruiting that apply DBS to the nucleus accumbens to treat addiction to opioids, alcohol, or methamphetamine.
Closed-loop brain-machine interfaces have been used successfully with DBS to treat movement disorders like Parkinson’s. Activity in movement-involved brain regions is recorded by an electrode, and a critical signal triggers an electric current to reduce tremors. A recent preclinical study used a similar responsive intervention in rats to control pain, and a model for using such an approach in addiction was provided in a recent small pilot study using deep brain stimulation in the treatment of two people with binge-eating disorders. Brain activity associated with food craving triggered the delivery of electrical current into the nucleus accumbens and quelled their cravings. Over six months, the participants experienced improved self-control over their eating, and they lost weight.
What if brain regions that control drug cravings could be targeted in real time, right when an individual recovering from an addiction was experiencing triggers and was in danger of relapsing? Better yet, what if we could do it without the need of planting electrodes?
One of the most exciting recent advances in neuromodulation is a method that uses low-intensity focused ultrasound instead of magnetic fields or electric current. Unlike those approaches, ultrasound can target areas deep inside the brain but is totally noninvasive. Focused ultrasound is already FDA approved in treating tremors associated with Parkinson’s, and trials are being conducted using low-intensity ultrasound to treat people with opioid-use disorder.
Closed-loop brain-machine interfaces utilizing ultrasound could potentially open up a whole new terrain of addiction management, one that could perhaps even involve wearable devices to deliver needed intervention in real time.
Could such an approach offer a potential cure for substance use disorders? Maybe, one day. And it is only one of many exciting avenues of research being pursued to address the current crisis. These novel technologies provide great hope for the millions of people who struggle with addiction in America and worldwide.
“Let us use whatever power and influence we have, working with whatever resources are already available, mobilizing the people who are with us to work for what they care about.” – Margaret Wheatley
The title of this post is inspired by Margaret J. Wheatley, Who Do We Choose To Be?: Facing Reality, Claiming Leadership, Restoring Sanity (2017). The book came up last year in conversations I had with Phil Valentine of CCAR when we were talking about influential readings. He told me about it and suggested to me it was to be digested slowly. I am an avid reader and sat down to read it from cover to cover. The truth of his words became clear to me after a few pages. Wheatley talks about how all things – even societies, have life cycles and that ours was in a period where large scale change is not often viable. Our institutions have decayed in the current stage in our society that they are largely ineffective at broad systemic change.
She suggests focusing locally and developing leaders to create space to support healthy community. I confess to not yet having finished her book. Having read books like Putnam’s Bowling Alone, The Fourth Turning by Strauss and Howe and Collapse: How Societies Choose to Fail or Succeed by Jared Diamond the topic is not new, but her focus (as far as I can see from about one halfway in) is to encourage leaders to develop and support community in ways that nurture people through difficult times. She calls these spaces “Islands of Sanity.” Quite a lot to digest. Truth be told and 15 months later I still have not finished this book even though it has had a great deal of influence on my thinking.
Many of us have experienced and are building such Islands of sanity in the recovery community. The Punta Gorda, Florida CCAR Multiple Pathways of Recovery Conference is such a gathering of people from around the nation to nurture recovery community. I have has similar experiences at the Mobilize Recovery convening in Las Vegas. The Association of Recovery Community Organizations through Faces & Voices of Recovery is another similar space. A theme of the conversations with people at these events is what do we do next to support additional recovery communities – I would call islands of healing around the nation. I think history has a few lessons for us on what works:
Communities can and do best self-define their own manners of healing. One of the well-known stories I have heard Don Coyhis, founder of White Bison and the Wellbriety Movement talk about is a conversation he had with federal grant officers when his organization was initially awarded funding to support recovery for indigenous peoples over twenty years ago. He was told he had to use evidence-based practices in the grant. He noted that the Native American community had several thousands of years of evidence of what worked to heal their communities. Much to their credit, they listened not just to Don, but to other recovery community organizations in including their own expertise in strengthening their own communities. In this way, these grants helped form these islands of healing across America through the SAMHSA the initial Recovery Community Support Project grants. These are community up, not government down solutions that can greatly benefit from the support of the government but must be led by the recovery community. Look at what was accomplished, the approach worked. CCAR and many other RCOs who formed at that time are evidence of this very dynamic.
If we want to build community-based services that meet the needs of our recovery community, we have to design funding around what works for these communities instead of trying to adapt healing processes to existing funding mechanisms. Recovery history shows us we tend to move away from community-oriented solutions as programming becomes institutionalized. We shift to fee for service funding models focused on individual units of care, following a clinical mentality. Instead of developing a deep understanding of what actually works, community-oriented programing is thus altered to meet existing funding mechanisms. These funding processes tend to favor large entities not grounded in recovery community. Community based recovery organizations try and use these funding mechanisms to serve their missions, but it often becomes a challenge as the focus becomes chasing these limited dollars and narrowing their missions to get paid for service units designed for clinical services.
There is great interest in the national recovery community to build additional communities of healing. Many of my conversations with leaders nationally end up focusing on what we can do to advance efforts to heal communities using a recovery community up model. As I have mentioned in prior articles, I see a lot of room for consensus, but that the development of such consensus involves deep conversations, inclusivity and a lot of active listening. Readers of this post inside of government seeking ways to address our burgeoning addiction epidemic would do well to follow the wisdom of leaders like Dr. H. Westley Clark and the first grant officer of the SAMHSA RCSP grants Cathy Nugent who worked to bring these communities together and to start building these bridges of healing communities by listening to their experiential evidence of what works and helping to support them instead of redefining them to fit into some other model.
There are many of us across the county invested in building a care and support system that actually meets the needs of our respective communities. When I see the depth of interest in this issue, it brings me hope. Our mutual well-being will be largely dependent on how we can help nurture each other’s islands and support new islands built by people focused on healing their own communities. In a post titled Creating a Broad & Inclusive Recovery Plank I suggested that developing broad goals is a good place to start strengthening such bridge building efforts.
Perhaps we should form a recovery island bridge building coalition of similar minded communities that want to understand and develop common ground in between our islands and build bridges that span our differences. Here are three points to start such a conversation:
Recovery communities are the experts on what is needed in their own communities. Recovery communities are diverse, and our efforts must be supported and funded equitably designed by us to serve our own communities.
Discrimination and stigma against us must end. Systems that tokenize us are perpetuating discrimination. It is not acceptable to tokenize our voices. There has to be an accounting for how this has happened historically to marginalize us in order for healing to occur and for our society to reap the full benefits that a recovery orientated model of care can offer.
How we do things matters. Our recovery communities are quite often vulnerable, and there are many groups, including some run by people in recovery that take advantage of our own people for material gain. We must establish a shared set of values and ethics and adhere to them to protect the most vulnerable among us.
So, to all the bridge builders of islands of recovery community – let’s find ways to develop consensus and understanding of each other and our experiential wisdom. If you disagree with my three points, I would love to hear yours, if those of us invested in bridge building listen to each other in this way, we will identify a common pathway forward!
It is true that when we come together, we are stronger. It is also true that the history shows us that we are most effective when we do so, even as there are so many forces that keep us arguing over small things. The truth is we do not need to have strong institutions to build consensus and community, we can do that with and for each other.
Please consider being a bridge builder between recovery communities, the island you strengthen may well be your own!
The addiction and overdose crisis in the U.S. continues unabated, with more than 46 million people having a substance use disorder (SUD) in 2021 and more than 100,000 people dying from drug overdose annually. And the crisis is increasingly hitting adolescents. Fentanyl, the main driver of overdose deaths, is now contaminating other illicit drugs including methamphetamine, cocaine, and counterfeit prescription pills, which may be taken by people, including young people, who have no prior exposure to opioids. Adolescent overdose deaths more than doubled from 2019 to 2021 (and deaths from fentanyl nearly tripled) after having held steady at relatively low levels for years.
The urgency of this public health crisis and the escalating danger of the illicit drug supply point to a need for a greatly expanded focus on prevention. Thanks to decades of research, we understand the environmental factors in childhood and adolescence that raise the risk for later substance use as well as the modifiable factors that can help protect against that risk and promote resilience. Effective interventions built on this knowledge range from nurse home visitation of disadvantaged first-time parents and pregnant women to various kinds of family- and school-based programs to build emotional regulation and self-control skills in preadolescents, teens, and young adults.
Many of these interventions have proven very effective in randomized trials—reducing later drug use, even in some cases by the children of the children who received the intervention. In fact, prevention interventions in childhood address risk factors for various psychiatric problems, not just SUD. Some interventions have been shown capable of mitigating the impacts of adverse social environments like poverty on brain development. Moreover, studies have shown that some evidence-supported prevention programs are extraordinarily cost-effective, an outstanding investment for communities over the long term.
The problem is, prevention interventions don’t get used enough. Important reasons include lack of will, as well as fiscal shortsightedness, since the benefits from prevention interventions are delayed from the time of implementation. But another major impediment is a lack of dedicated infrastructure and workforce for prevention. For example, school systems that wish to implement prevention programs turn to teachers who likely have not had any prior training in substance use prevention, and already have numerous competing needs. This is further exacerbated by other educational curriculum requirements taking precedence in time allocation over prevention.
And unlike substance use treatment, which may be covered by private insurance or Medicaid, there is little in the way of dedicated funding for prevention. A prevention program may need to be paid for by cobbling together funds redirected from other priorities. It severely limits the reach of potentially effective interventions and means they are unlikely to be sustained over time if they are ever taken up in the first place.
Policy changes that would place increased priority on preventing substance use and its consequences and increase public funding for it could help increase the reach of prevention and help mitigate drug crises like the one our country is currently experiencing. But as my NIDA colleagues Drs. Amy Goldstein, Barbara Oudekerk, and Carlos Blanco highlight this month in Psychiatric Services, prevention researchers can also do more to ensure that interventions they design can find a home in the various systems that could implement or pay for them. That means developing and testing interventions in the settings where they are intended to be delivered and designing prevention programs that meet criteria that would qualify them for funding under the Patient Protection and Affordable Care Act (ACA), child welfare, or federal prevention dollars administered by the Substance Abuse and Mental Health Services Administration.
For instance, the ACA requires that preventive services be completely covered by insurance as long as they meet certain standards of evidence set by the U.S. Preventive Services Task Force (USPSTF), but those standards are currently only met by a small handful of prevention interventions. The USPSTF identifies gap areas in the evidence, so NIDA’s prevention research is now funding research that could generate the evidence needed to redress those gaps.
Greater collaboration between prevention researchers and those in a position to fund prevention programs could facilitate developing interventions that have greater promise of being paid for and sustained and that are more responsive to community needs. It could also spur innovation and even the development of new interventions in less traditional settings like justice systems and new strategies that take advantages of virtual tools and wireless devices.
As a society, we must do much more to foster mental health and resilience in young people as well as screen patients at all ages for potential or emerging drug problems before addiction becomes their reality, and before drug experimentation escalates, creating havoc in a person’s life or even claiming it. Prevention, if properly implemented in universal and tailored settings, could play a much larger role in reducing the numbers of Americans with drug addiction and stemming the tide of overdoses. For that to happen, the science of prevention should tackle strategies that address the challenges of paying for and delivering prevention services in a world with competing public health priorities.
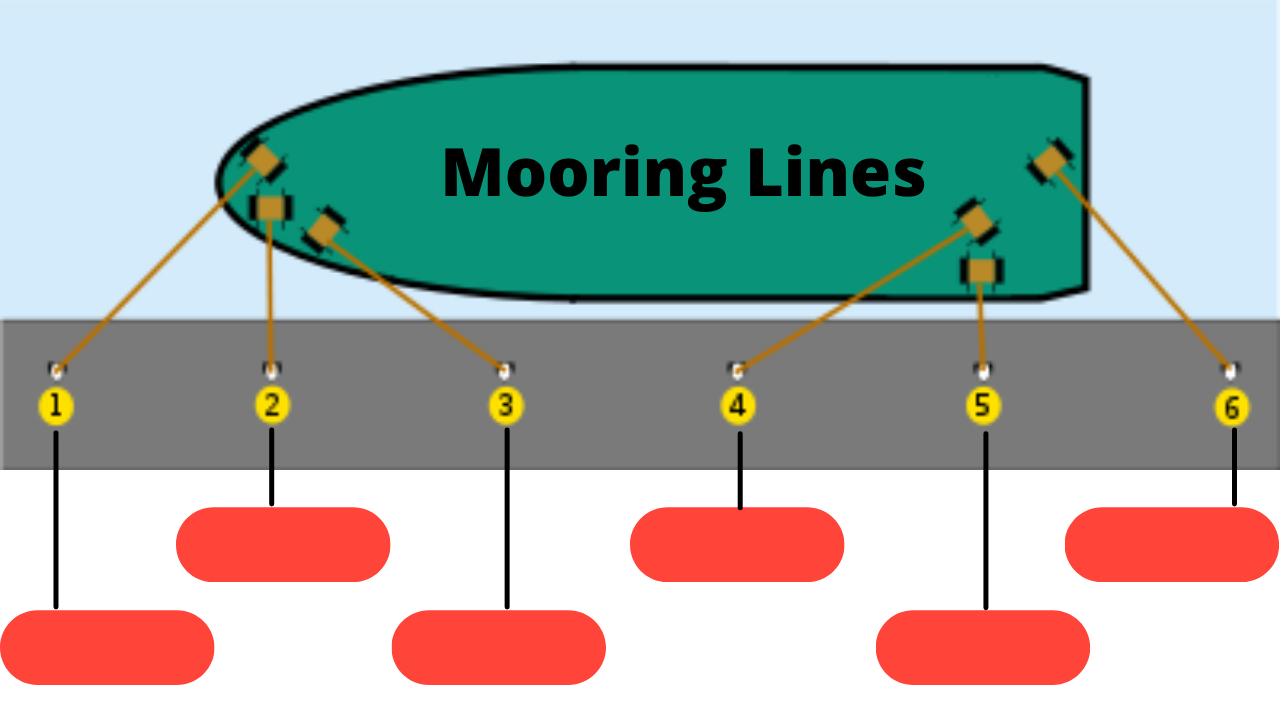
[Ed. note: Although Mooring Lines are not an “official” SR Tool, volunteer Stefan Neff and others have found them very useful in their recovery. This post represents Stefan’s views and analysis.]
I was recommended to use a process called Mooring Lines by a counsellor who said this tool is an important concept in addiction recovery. Also, the Substance Abuse and Mental Health Services Administration (SAMHSA) has recognized Mooring Lines as a helpful tool for individuals who are struggling with addiction.
What are Mooring Lines?
Mooring lines are metaphorical anchors that individuals can use to ground themselves when they are feeling overwhelmed or triggered by their addiction. They are a set of personal values, beliefs, and practices that provide stability and support during difficult times. Mooring lines are created by identifying the things that are most important to an individual and then creating a plan to prioritize and protect those things.
How Do Mooring Lines Work in Addiction Recovery?
Addiction recovery is a challenging process that requires individuals to make significant changes in their lives. These changes can be difficult to sustain without a solid support system in place. Mooring lines provide a framework for individuals to identify their values and beliefs and then use them as a foundation for their recovery.
Mooring lines can be used in a variety of ways. For example, an individual might use their mooring lines to remind themselves of their commitment to sobriety when they are feeling tempted to use drugs or alcohol. They might also use their mooring lines to reconnect with their spiritual or religious beliefs, which can provide comfort and guidance during difficult times.
Benefits of Mooring Lines in Addiction Recovery
Mooring lines offer a number of benefits for individuals in addiction recovery. Here are just a few:
Increased Self-Awareness: Mooring lines require individuals to reflect on their values and beliefs, which can help them better understand themselves and their motivations.
Greater Resilience: Mooring lines provide a stable foundation for individuals to rely on during difficult times, which can help them weather the challenges of addiction recovery more successfully.
Improved Decision-Making: Mooring lines can help individuals make better choices by providing a clear set of priorities that guide their actions.
Increased Motivation: Mooring lines can provide individuals with a sense of purpose and direction, which can increase their motivation to stay sober and continue on the path of recovery.
Mooring lines are an effective tool for individuals in addiction recovery. By identifying their values and beliefs and creating a plan to prioritize and protect them, individuals can create a stable foundation for their recovery. Mooring lines can help individuals stay focused on their goals, make better decisions, and stay motivated during the recovery process.
Mooring lines Examples: Journaling, mindfulness/meditation, SMART meetings (therapy & case management appointments in some cases), recovery research (Sober Friends Club), exercise, diet, sleep and others.
Now make a list of your own mooring line that will help you stay grounded and connected to your recovery or sobriety path.
In 2005, concerned at the lack of choice in addiction treatment in Scotland and hearing frustrations from patients and families around lack of access to residential treatment, I sought support and funding to set up a drug and alcohol rehab service based on the therapeutic community (TC) model. This would be unique in Scotland as, based in the NHS, it would be free at the point of delivery, eliminating difficult funding pathways.
I proposed the service should serve a local population to keep people close to their families and allow them to develop local recovery supports and access intensive aftercare. It should develop close working relationships with other treatment and support options – this should be an ‘as-well-as’ service rather than an ‘instead-of’ service. There should be direct family support and detox offered as part of the deal. We would actively connect people to recovery resources in the community, offer them peer support and open avenues into education, training and employability.
Outcomes from rehab in Scotland (and even the UK) at the time were hard to find – but so were any treatment outcomes from services already in operation, so I built in that we should commission a robust evaluation. If this wasn’t going to work, we needed to know that – and if it helped people achieve their goals we wanted to get that message (and any other learning) out there.
This proposal and the evaluation were funded for a two-year pilot and in 2007 LEAP was born. A lot of people then came on board to help transform an idea into a reality. A little delegation of addiction doctors approached me as soon as the funding announcement was made. They were worried that by encouraging people to seek an abstinent recovery, we would end up putting them in grave danger. I pointed to the mitigations we would build in, we would ensure that potential risks were discussed and that consent would be fully informed. I’m not sure that I convinced them all, but in time some of these colleagues began to refer patients to us.
A very scrutinised service
So what of the analysis of the service?
Our initial evaluation was conducted rigorously by Figure 8 and the one-year 170+ page report shared with the commissioning ADPs and the Scottish Government shortly after a year of operation.
The two year report followed in 2010.
In 2014 we did a ‘Road Tour’, visiting Glasgow, Edinburgh and Dundee to disseminate the four year (as yet unpublished) outcomes.
The one-year outcomes were published in a peer-reviewed journal in 2017.
Our four-year outcomes have just been published in the British Journal of Psychiatry (Open) Journal this month.
After the initial baseline data collection, follow up was done by external researchers. Our family programme and recovery house have also undergone rigorous external evaluation.
So, in effect, quite a lot of scrutiny of what we’ve been doing – not to mention the data that has been reported regularly from the outset to the present day to the three Alcohol and Drug Partnerships that commission our service. What does all that data mean? Are there any key messages or things that are worth passing on?
The detail is in the published papers, but I think there are some valuable higher level lessons across the years that these reports and papers span. I want to share some of this because the learning has helped us, our patients and their families. It undoubtedly has wider implications.. What I’m sharing is based on research evidence, evaluation, plus a little bit of experiential learning too.
You can establish and run a rehab in an NHS setting
Not everyone thought that the NHS (in partnership) could run an effective rehab programme. The premise was simple: services to aid recovery from addiction should be available on the same basis as services for cancer, diabetes or broken bones – comprehensive and free at the point of delivery.
Until recently, to access rehab in Scotland you had to live in the right area, be wealthy or just lucky. Our initial evaluation gave us affirmation that an NHS service and its partners could deliver a service of high quality with good outcomes – joined up to other NHS services.
Lesson: there are advantages to embedding drug and alcohol rehab in the NHS as part of a recovery-oriented system of care.
Demand – if you build it, they will come
Lothian had few referrals to rehab per year prior to LEAP. It would have been easy to say ‘there’s no demand’, yet within a short space of time, a waiting list for rehab treatment developed which then doubled within a further year. Despite 16 new beds being available locally in Edinburgh for Lothian referrals, demand was quickly outstripping supply.
Lesson: when you value rehab and have straightforward pathways to it, referrals roll in.
Rehab associated with improvements in various life domains
We did find evidence that attending our programme was associated with improvements in a variety of outcome domains and that those who stayed longest/completed had the greatest gains. The two published papers capture this in detail.
Lesson: we can be optimistic that rehab is likely to help a significant number of people reach their goals.
Retention is important.
The best outcomes are for those who complete – our evaluations and our study have clearly demonstrated this. We adjusted our practice based on this finding to help the maximum number of people get to the end of the programme. Retention in the early days was around 55% (which was still better than the average for a 90 day programme in the UK), but we’ve increased this to around 65%.
We have a really high threshold for discharging people and we have instituted measures associated with treatment completion. We’ve found that tailoring the programme, varying the length of it, using contingency management, peer support and a variety of procedures to manage challenging behaviour short of discharging people work well.
Lesson: we need to pull out all the stops to get people over the finish line (and the finish line is not the finish line in any case…)
Deaths
Deaths in this rehab population were not related in time to detox and were more likely to occur from respiratory disease (a quarter) and complications of alcohol dependence (a third) than be drug-related. That doesn’t mean we are complacent. We instituted measures like raising our methadone threshold (to avoid people detoxing too much in the community prior to admission), inpatient partial detox, naloxone distribution, overdose prevention training, rapid referral back into MAT where return to use occurs, offering inhouse re-titration onto OST to those leaving early etc.
Lessons: the risks associated with opioid detox can be mitigated in this setting. It’s important to look after general health.
The severity of dependence does not predict outcomes
The LEAP study cohort at intake was older than the average treatment seeking population (34 vs 27), had higher drug and alcohol use and more severe alcohol and drug problems as measured by the severity of dependence scale than in the Scottish DORIS cohort. However the severity of dependence did not seem to predict treatment outcomes.
Lesson: don’t deny a rehab place based on how severe someone’s dependence or problems are – you may be surprised.
Rehab can impact on injecting behaviour
In our study we divided our patient group into those who completed vs those who did not complete and compared the two groups. In those who completed there were significant reductions in injecting behaviour (though we need to be cautious as numbers were small).
Lesson: rehab is effective harm reduction
Rehab can generate significant cost savings
Although health economics is a notoriously difficult subject, our evaluators noted:
“This report suggests that the costs incurred in achieving recovery outcomes for LEAP graduates are more than offset by the savings across health and criminal justice domains by a factor of as much as 3.”
Lesson: rehab can make significant cost savings downstream and may be more cost effective than other treatment options in the long term.
Abstinence is associated with better outcomes.
Abstinence is not everybody’s goal, but in our patient group, those who achieved abstinence did best overall – something in keeping from research elsewhere. It’s been my experience as a professional that abstinence as a goal is not well received or supported in some circles, yet undoubtedly it is something some people coming for help want and something that significant numbers of people can achieve (More than 60% of those who completed treatment at LEAP reported abstinence at 4 years in our study).
Lesson: abstinence is a legitimate and achievable goal, associated with good outcomes.
Other lessons
There are other lessons we’ve learned: the recovery journey can be long and non-linear, so rehab makes best when it’s joined up to a robust system of care. The therapeutic community is a powerful force for change. There’s no need for a battle between harm reduction and abstinent recovery when the larger system you operate within offers both and referrals happen in each direction depending on need.
Hope matters – lived experience in the staff team and from peer volunteers really helps here.Harm reduction measures are simple to adopt into rehab settings. Effective and fast referral back into community treatment is important when people return to use. Intensive preparation and long-term aftercare are vital.
A multi-disciplinary team allows us to accept those with greater needs. Addressing mental health is critical to success. People have multiple co-morbidities. Polypharmacy can be effectively addressed in rehab. People are often able to go on to do longer term therapies for PTSD. People may need more than one rehab treatment episode, so ‘one shot and you’re out’ makes no sense. When patients benefit from rehab so do families, but families also have the right and opportunity to find their own recovery and support can be provided in-house by the service to achieve this.
Summary
Residential rehab should be part of a comprehensive care system – the time for saying ‘there’s no evidence that it works’ is over. Yes, it’s only a part of the recovery journey for some, not all, and yes, it’s not something everyone wants. But some people do want rehab and they ought to have a choice about it. It is possible to deliver rehab in an effective manner with good outcomes, including harm reduction outcomes for the people who go through it. Furthermore, as the evidence accumulates, it’s possible to improve the quality of the services we offer.
Rehab is effective and can be a powerful tool to help those with addictions reach their goals.
I’d like to thank all of those who gathered and examined evidence for our service – Figure 8, McMillan Rome and the authors of our two peer-reviewed papers, but particularly Dr Nina Mackenzie for her part in our four-year outcome paper. Thanks are also due to the amazing LEAP team and volunteers, NHS Lothian, our colleagues across statutory and third sector services, our partners (City of Edinburgh Council, Access to Industry, the Cyrenians, The Ritson Clinic, the Lothian Alcohol and Drug Partnerships and the Residential Referral Team) and, most of all, to our patients who have achieved remarkable outcomes through their determination to recover and via the hard work they put in.
The drunk driver crossed the line and changed Kristal Field’s life forever. She was seriously injured and her best friend was killed. She required opiates for pain relief and struggled for the next ten years, crossing her own line at some point from taking opiates for pain management into full-blown abuse. Kristal lost herself in a cycle of misusing opiates and her life became focused on feeding the addiction. It all came to an end with her 2013 arrest for possession of narcotics. That’s when the rebuild started.
Because it was her first arrest, Kristal was put through a diversionary program that included being sent to Narcotics Anonymous (NA) meetings. Nobody mentioned other options like SMART. Kristal says she had trouble with the idea of a “higher power” that is integral to 12-step recovery like NA, but she figured out how to stick around, “The way I chose to think about [higher power] is that it was the fellowship, it was the group, it was the sharing of information…hearing other people’s stories, that is so powerful in itself.” This strategy kept her life moving in a positive direction, even as she remained convinced that she did have power over some things and there were things she could control.
One example was her decision to pursue a college degree, and that led her directly to investigating SMART for a class assignment. It clicked, “I absolutely just loved everything about it…it resonated so much with me and was also in alignment with the things I was doing in school.” Kristal started attending meetings and found it personally valuable as she juggled working full-time, going to school, being a mom, and being in a relationship. She also attended Family & Friends meetings, which she credits as helping mitigate her household’s COVID pandemic stress.
The next powerful decision she made was to become a SMART meeting facilitator. As a self-identified introvert, Kristal says stepping into a facilitation role was definitely out of her comfort zone, but she did it anyway and was rewarded, “Going through the facilitator training was life-changing, it made so much sense and it really made it all come together for me in my own recovery.”
Now Kristal looks ahead and realizes that with her Human Services and Health Administration degrees, combined with her SMART Facilitator training, the sky is the limit. “My ultimate dream would be to open my own recovery house and if I could run SMART meetings all day every day that would be great!” She says watching participants grow, even through tough times, is rewarding. Kristal particularly relates to the women members of her group learning how to advocate for themselves and use SMART tools to develop the strength to do so. She sees it happen regularly.
Ultimately, Kristal just wants to see SMART grow as much as possible, and help individuals before it’s too late. She has lost friends to Opiate Use Disorder, but now she is part of the solution, “I may not be able to bring my friends back but I can still try and influence the ones who are still here.”