

Forward: We have a long and rich history of recovery in America. It is vital to understand the effort that has gone into providing avenues into recovery. It has taken an incredible effort over many generations to get us as far as we are in respect to eliminating disparate care and discrimination, improving access to care and providing support for our families and friends. It is not nearly enough. Far too many of us are still dying from this common yet highly stigmatized condition. In the spirit of recovery, I have taken on this project to document the perspectives of leaders who attended the 2001 Recovery Summit in Minnesota. A name that kept popping up as playing a pivotal role in making it all come together was William Cope Moyers of the Hazeldon Betty Ford Foundation. I can see why having conducted the interview below.
One of the things I had the opportunity to do was to relay to Mr. Moyers what the work he has done and the efforts his parents made to initiate a much-needed conversation about addiction and the family. For those of you who were not around, it would be hard to convey the deep connection many Americans have to his father, Bill Moyers. It is a name trusted across the nation. Moyers on Addiction: Close to Home first broadcast in 1998 and it sparked a national conversation that was long overdue in America. Addiction remains an issue steeped in taboo and deep shame. I have no idea what it must have taken for his parents to produce a special on this issue that had such an impact on their own family. They broke the unspoken rule that must be broken – they talked about addiction and relapse and recovery and the science of addition and how stigma gets in the way of people asking and getting help. They presented it in a way that opened up people’s minds. I asked him to thank his parents for their significant contribution they made to this dialogue. I saw its positive influence in my community after it came out. He told me that would mean a lot to his parents, and he would let them know their contributions are so deeply appreciated.
William C. Moyers is the vice president of public affairs and community relations for Hazelden Betty Ford, based in Minnesota. As the organization’s public advocate since 1996 Moyers carries the messages about addiction, treatment and recovery to audiences across the nation. He has appeared on Larry King Live, the Oprah Winfrey show, Good Morning America and National Public Radio. Moyers is the author of several books including Broken: My Story of Addiction and Redemption, a New York Times best-selling memoir published in 2006 that is still in print. He lives in Saint Paul. He has written several books on addiction in recovery including Carrying messages of addiction, treatment, and recovery, A New Day A New Life Journal and the DVD Broken Softcover: My Story of Addiction and Redemption and Now What: An Insider’s Guide to Addiction and Recovery.
As he notes in his interview, he is still a journalist at heart, and I want to acknowledge that it was a little intimidating interviewing a person who is a master of the craft. It is also true that the bond of recovery came through the phone line as we compared our individual journeys and the insights we have learned along the way, and we talked briefly about our mutual interest in addiction policy. It should be no surprise that Mr. Moyers was as gracious and as humble as everyone else I have interviewed in this project.
- Who are you and what brought you to St Paul at that time?
What matters the most is that I am a man in long-term recovery from addiction to alcohol and other drugs. I have been in recovery since 1994, when I had been living in Atlanta and working as a journalist for CNN. Starting in 1989 with my first treatment, at Hazelden, I had experienced periods of recovery prior to that, when I sought help at that time, It became important to me to move back home to Minnesota which I did when I got out of treatment. I blundered into a job at Hazelden, as we were then known, in 2014 we merged with Betty Ford and became the Hazeldon Betty Ford Foundation (HBFF). They were advertising an open policy position and I ended up getting the job even though I surely wasn’t the most qualified of the applicants, and there were hundreds. This part of the story is germane to everything that came after in Saint Paul. When I took the position, my call to action was to change public policy around substance use treatment, expand access to care and to address stigma associated with addiction. What a tall order!
It felt daunting to me, and I did not know anyone doing that kind of work. HBFF is a healthy nonprofit and we are able to do some really great work, but we are still a nonprofit. Our funds were limited and the scope of what needed to be done was overwhelming. I knew we were going to need to draw a lot of people across the country into this call to action. I had no idea how to do it. About a year later, in 1996 I was asked to give my first public speech at my local rotary club in Saint Paul. I was a member. I was not going to let my fellow Rotarians down. Of course, I said yes.
The topic I was given was the impact of alcoholism in the workplace. I spent weeks researching the facts and stats and crafting them all into a speech I figured would resonate with the audience. My presentation came after lunch, and I got up and started to do my presentation to this group of 200 people. As I was delivering my speech, I realized I was losing them. The audience was falling asleep, and it was not because they just ate lunch. They already knew the things I was telling them, and they just were not that interested in hearing me share about the impact of alcoholism in the business sector. I decided I had to do something radical to get their attention again, and I decided on the spot the only thing I could do was shift gears. I decided on the spot as I stood at that podium, I would tell them what I knew about addiction and recovery in the workplace from my own life experience.
I abandoned my prepared speech and I started to speak off the cuff about my journey into recovery and the experience of my parents, Bill and Judith Moyers. I told them about my four treatment episodes over five years and how I got into recovery and rebuilt my life and the impact it had on my family. My parents were not aware of my addiction as it unfolded. They did not know what to do to get me help or anything about the challenges we would all face on the journey of recovery. My father Bill Moyers was a public figure, a broadcast journalist and my mother Judith Moyers was a executive producer for the family’s television production company in New York and our story, even though I come from a well-known family was a familiar one to many Americans, including the audience on that day. However, it was not a topic people talked about openly. That day, I spoke about the power of recovery and resiliency without focusing on the ugly details that come with addiction. You could hear a pin drop in that room.
As I stood there and told my recovery story, I realized the power of storytelling. I realized that sharing hope helped people to feel empathy about this deeply stigmatized condition. A few things came out of that experience. I had a sense that story telling could help shift public perception about addiction and recovery. The second thing that happened is that I became a beacon of hope for people in my community. People who had attended the lunch started calling me for help. A few days after the presentation a man showed up on my front porch trying to get help for a family member. Things like that began happening all the time. The magnitude of need became deeply apparent to me, and it redoubled my commitment to the mission I was called to do. I was more determined than ever to serve that call to action, to change public policy around substance use treatment, access to care and to address stigma associated with addiction. At this time, I thought I was alone. I thought I had found something in storytelling that nobody else knew, I didn’t know anybody else was doing this kind of thing. Later, I came to find out that there were pockets of people around the nation who were doing the very same thing.
It wasn’t long after, maybe a year or so, through their independent production company, Public Affairs Television my parents put together a five and a half hour, five part series on addiction called Moyers on Addiction: Close to Home. It was one of the first docuseries that spoke to what was happening to families all across America, including our own. I had a very limited presence in the series, like two minutes. However, it was such a relatable story that people were intrigued about me and saw the story as one that was playing out in a lot of families across America. People began to associate me with the topic, and I started to connect with people like Johnny AllemSis Wenger of NACoA, Stacia Murphy of NCADD and Bill White. It provided a platform for me to work on this call to action, which was clearly bigger than HBFF and one that resonated deeply with people.
There is an element of this story I don’t think people know about. One of the groups we connected with was the Robert Wood Johnson Foundation (RWJF). They had done some of the outreach for Closer to Home and they were very focused on addiction and recovery at that time. I got an invitation to present ideas on what was needed in the treatment and recovery space and an audience with the President and CEO of RWJF, Steven A. Schroeder. Through some of the connections I had been making I realized we had an opportunity to build a recovery movement. I knew that what needed to happen had to be framed around recovery and not treatment. I took Jeff Blodgett who had been the campaign manager for Paul Wellstone to the meeting. He had just finished studies at the Kennedy School and needed a job, so we hired him despite not having much money. We went to Princeton New Jersey together and met with the people from RWJF. We presented the idea of a summit to start to connect all of these groups across the country under what we called the Alliance Project. They thought it was worthy and they gave us a half million dollars. This was a lot of money at the time, particularly in the addiction and recovery space where such philanthropy is still not very common.
As I mentioned, we started to realize there were pockets of people all across the country who were advocating for recovery. I thought I had discovered something others did not know back when I shared my recovery story from that podium at the local rotary club. What I learned what that there were a lot of people around the nation who were doing very similar things. People coming from a place of humility and service and working really hard to change public perceptions about addiction and recovery. Working to save lives. We started to pull them together and we had help from people like Johnny Allem who had run Society Of Americans in Recovery (SOAR) and Paul Samuels who ran the Legal Action Center. We realized that these people where the drivers. We wanted to bring them all together and convene a summit. That is how it was born. That is what helped bring together the elements of what we now know twenty years later as the New Recovery Advocacy Movement (NRAM).
- Is there a particular moment or memory that stands out to you from that summit?
There are actually two memories that stick out to me. The first occurred in the weeks that preceded the summit. It was right after 911 and the horrific terrorist attack on our nation. I was standing in my back yard having a phone conversation with Jeff Blodgett. I recall standing there and watching fighter jets providing air cover over the twin cities of Saint Paul and Minneapolis. I recall thinking that this is as close to war as I had been in my whole lifetime. The conversation with Jeff was on whether or not we would proceed with the summit, and it got rather heated. I was thinking that there is no way we could do it. Jeff was arguing that we absolutely needed to move forward. My sense in retrospect is that a lot of the people we invited from around the country were with Jeff on that issue. He was right. We moved forward despite the uncertainty that everyone was experiencing across the country.
The second memory was on the last day of the summit, a Sunday. It was clear that what we all put together was resonating with people. Something big was happening, we brought the right people together and things were resonating. We could all feel the energy in that moment. I was walking through the ballroom area, which coincidentally was the same space I had given that first speech to the rotary club a few years before. A television was on. It was Sunday, October 7th, 2001. As I walked through the room, I heard President George W Bush. He was on the television announcing to the world that Operation Enduring Freedom (OEF) had started with airstrikes in Afghanistan that very morning. I realized we had pulled it off, we had conducted the summit in between the 911 attacks and the start of war. It was in the nick of time, and we managed to get it done.
- What did you see as the motivating factors that brought you all together for that historic summit twenty years ago?
As I had spoken about earlier, we saw the call to action as something that had to focus on recovery, not treatment. One of the things I am really proud of is the behind-the-scenes role that Hazelden had played in the summit. Hazelden had agreed to serve as the fiscal agent for the initial RWJ grant the money provided us by RWJF. One of the untold facets is how we handled that money. Everything was covered for all of the participants travel, food & lodging. While Hazelden put a lot of effort into the project, we only kept $1 for our role in bringing it all together. It was a symbolic dollar. I think people in recovery will understand that a lot of what we all do is motivated by a deep commitment to service. The work that was done to put the summit together was entirely consistent with the mission of HBFF. It is important to note that we were all motivated by a sense of commitment and service and the dire need to change how America saw addiction and recovery. Looking back, what I hope people realize is that part of what made it all work is that everyone left their personal or organizational agendas at the door. We worked on this call to action as a common area of focus. We worked to bring these advocates together and find common ground. We worked to give recovery a voice in public policy. We worked together to change how America sees addiction and recovery. That dollar was part of how HBFF demonstrated in a concrete way how important we saw this effort. In short, we were all motivated by a deep sense of purpose to the cause of recovery in America.
- How have we done in accomplishing those early goals?
We are STILL HERE! What an accomplishment that is in and of itself. Faces & Voices of Recovery started to form out of this effort and twenty years later it is still here too! There is a greater understanding of recovery through the power of personal story. We have more effective ways to communicate the power of recovery. It is easier for people to talk about addiction and to seek help than it was before the summit and what emerged out of it. These are huge things. Work on policy issues like the Mental Health Parity and Addiction Equity Act (MHPAEA) got signed into law and probably would not have even been possible without these efforts. But the most important thing we did is show the world that when recovering people come together in common purpose, great things happen!
- What do you see our greatest successes to date are?
As I noted, we are all still here. This is no small accomplishment. There have been many attempts to create such a movement in the past. SOAR is an example. There was an event here in Minnesota called FreedomFest 1976: A Celebration of Freedom from Alcohol and Drug Addiction that headlined Dick Van Dyke. 20,000 people attended, many of them open about their recovery. So many people where there. Don Newcombe, Art Linkletter, Garry Moore, Senator Harold Hughes, Virginia Satir and many others. There is this deep reservoir of recovery across America that has been around for so very long but we have always had difficulty coalescing and coming together. At the time, all the elements seemed to be present, but the timing just was not right. There are internal and external forces that have pulled apart such efforts. Our greatest success is that we are still here. We have sustained this effort over twenty years. That is a huge success. It might be fragile, it is probably something that will need a lot of tending to sustain, but we need to acknowledge what an amazing thing we pulled off collectively.
- What did we miss if anything looking back at those goals?
I think we have missed an opportunity to grow the movement through more philanthropy. If you look at major national organizations like the American Cancer Society or the March of Dimes or the Muscular Dystrophy Association, they harness significant private funding and deep community support. They have a lot of visibility, and it has helped drive public awareness, treatment and recovery processes for those conditions. We are not there yet. Faces & Voices has done some amazing work and other groups have also formed, yet we do not have the groundswell of support we need. We do not have philanthropists who want their names associated with our cause. Of course, this is a vestige of stigma, but for all of those other issues, there was a moment in which some deep pocket visionary decided that they would invest their resources in changing things despite all the barriers. We do not quite have that yet. Gary Mendell of Shatterproof has done a lot on behalf of families. We need others to step up an invest in our recovery community.
What we did do was a whole lot like throwing a handful of seeds into the wind and watching what took root. Some landed on concrete and stuck their roots into the cracks in the ground, others withered on infertile earth. Some landed in fertile soil and flourished and have even grown into forests. That is what we did, and it is so valuable, but a lot more work needs to be done to ensure better access to care, and end to discrimination and seats at all the tables we need to be sitting at. Stigma and discrimination are still such profound barriers. We have a long way to go and the way to accomplish it is broad community support that include benefactors willing to invest in our cause. Together, these elements would help create greater focus on the power of recovery to transform lives, families and communities.
- What are you most concerned about in respect to the future?
I think I am more concerned about our long-term impact than anything else. When I look around, I still see that people still have an incredibly hard time finding help. I get calls two, three or five times a week from people trying to get help for a loved one. We have long wanted to get to a place where access to care was seamless and timely. There is a short window for persons to get help. So much of that time is spent trying to figure out how to get in the door and then stay in care. I think we were right not leaning too much on the treatment system to build these bridges but instead should strengthening the community. We still have a whole lot of barriers. There is also a great need for basic ethics in our field. So much money flowing in but not necessarily focused on strengthening these foundational elements. Having a strong recovery community was what we envisioned as the foundation for this work. There will be a need to have a fresh set of leaders pick up this ball and carry it forward. Movements like ours have always been fragile and have always faced challenges. It will flourish when new leaders are nurtured and take what the prior generation did and carry the vision forward in ways that meet the needs of the times. I am concerned, but I am also quite hopeful.
- What would you say to future generations of recovery advocates about what we did and what to be cautious of / your wishes for them moving forward?
There is a quote that comes to mind from President John F Kennedy from a speech in 1963. He said that “change is the law of life. And those who look only to the past or the present are certain to miss the future.” It is important to understand the past and we must live in the present, but we also have to dare to dream about the future and work towards that vision. The truth that is evident when we reflect on history is that everything that we have in respect to addiction treatment and recovery support has come from our community. I am confident that for all the things we achieved, someone looked at the aspirations of those leaders in that era told them that what they were trying to do was simply not possible. They did it anyway. They refused to accept that the barriers were insurmountable. They worked as hard and a long as they had to make that vision a reality. That is our history. I hope it is our future as well.
I would tell these new leaders to step up. I would tell them to learn our history, to look around at what exist today and then decide what we should have and work as hard and as long as they need to so that the next generation benefits from the improved reality that they create. This is our story; this is the legacy all of were given by those who came before us. This is the path to the place we need to go. The call to action I was given when I got to Hazleton Betty Ford is not yet complete. We moved the ball forward. I would tell them to not settle for what is, but work towards the reality they want with the resources and tools we have worked hard to give them. I would tell them to do the work out in the community, not on social media. I would ask, if not them, then who? It has always been a long game we are playing. That is the road we walked. I know that they can do even greater things.
Prevention of substance use is probably more important than ever. And the relevance of prevention across the lifespan (including among those who have already initiated use) has probably never been more important.
Why would I say that?
The purity and potency of substances have increased so much that preventing even a one-time use of certain chemicals can now preserve the quality of life and be lifesaving work.
It now seems to me that Prevention should:
- be a service within every stage and level of care
- apply continuously across the lifespan, and
- no longer be a stage and kind of care that only happens before first use.
And it seems to me that all existing Peer Support and Harm Reduction specialists should be cross-trained in Prevention. (In that way we would not create the burden of adding Prevention-specialist staff to all services).
Why we all need to learn prevention
The new problems related to availability, potency, and addiction potential associated with:
- fentanyl, sufentanil, carfentanil, and novel high-potency opioids (e.g. causing death upon the very first use),
- novel high-potency benzodiazepine derivatives (e.g. causing complicated and hard-to-manage withdrawal; seizures; prolonged confusion after stopping use),
- novel high-potency methamphetamine derivatives (e.g. causing prolonged paranoia, irritability, and problems with decision making and impulse control lasting long after cessation of use), and
- ultra-high potency THC formulations (e.g. prompting onset of first psychosis; and psychotic episodes lasting days, weeks or months after cessation of use);
are serious and concerning.
In addition to the problems listed above, those illicitly selling substances now commonly add very high potency pharmaceuticals and novel synthetics to the street-level supplies of both prescription medications and “natural” drugs. Thus, today, one’s first use may no longer be to merely “try pot” but rather to “vape high-potency THC wax” – and accidentally die of an opioid overdose from the fentanyl the person did not know was in it.
The clinical presentations of these problems I have seen in recent years are dramatically worse than the problems associated with potency I saw in addiction treatment in the late l980’s through the 1990’s.
- Prevention should be added as a service within and across every stage and level of care.
- Prevention should apply across the lifespan.
- Prevention should no longer only be a stage and kind of care before first use.
- Existing specialists in Peer Support and Harm Reduction should be cross-trained in Prevention (rather than add Prevention-specialist staff to all services).
Classic Versions of Prevention
Prevention has typically focused on maintaining the prohibition against initiating substance use. This work has typically been focused on children and adolescents.
In that way, prevention was usually thought of as only happening before any use begins, and before harm reduction efforts are relevant. This is especially true when considered chronologically, or across the segments of a person’s lifespan.
That approach retains merit. Perhaps the simplest first reason to prevent initial use is what I have called the Harms of Use. For example, research efforts to quantify and scale:
- the wide variety of simple harms of simple use1
- physical harms, physical dependence, and social harms from substance use2
- genetic vulnerability to both simple harms and to addiction potential3, 4
- vulnerability to developing a substance use disorder based on the facts and circumstances of one’s life (e.g. Adverse Childhood Experiences), and
- years of life lost5
have been undertaken.
When I entered clinical work in addiction treatment back in the late 1980’s, the average addiction counselor I met knew that Prevention programs existed. But almost none of the addiction counselors I met seemed to know any specifics about what was done by the workers concentrating in Prevention.
At that time, Prevention as a field generally:
- centered on child and adolescent populations
- focused on primary prevention (preventing initial use)
- did its work in non-clinical settings (e.g. schools)
Prevention work was largely concerned with:
- promoting psychosocial health (e.g. self-esteem) and improving resiliency – as matters related to decreasing the numbers and rate of youth initiating substance use
- preventing initial use in the first place, especially among those for whom risk factors of SUD disease progression were present.
In that way, Prevention did not apply during active addiction illness, nor impact the course of addiction illness once the illness began.
Is that approach to Prevention sufficient today?
Classic Versions of Harm Reduction
Harm reduction (HR) in its classic formulation is centered in providing education, supplies, and related methods for safer use among people who already use substances or are experiencing addiction illness over a longer term. In that way, harm reduction is centered in lowering the negative effects of use. HR efforts can be implemented with:
- those who are experiencing simple use (and not a substance use disorder),
- for those with a mild use disorder, and
- those experiencing complex, severe, and chronic addiction illness.
During the late 1980’s, seemingly all the counselors I worked with or met knew about Harm Reduction approaches generally, including:
- the needle exchange and related education services we had in our city (that the Police in town knew existed, but did not target)
- the outpatient methadone maintenance program in town (which began operation in the late 1960’s, and I worked in for many years), and its graded responses to opioid use and use of other substance classes – such as cannabinoids or alcohol during methadone maintenance
- that the 1-2 year residential program (Therapeutic Community model) in town did not necessarily administratively discharge patients for alcohol use while on pass during the final (re-entry) phase of treatment
- the axiom that “We don’t kick the patient out of the respiratory ward for coughing.”
Is that Harm Reduction approach sufficient today?
A New Look at Some Old Ideas
Given the dangerously increased potency of many chemical compounds available today (especially compared to substances available when I started clinical work in 1988), some notions about the safety of use might be reconsidered. For example:
“Gateway drugs” is the common term for the idea that use of some less stigmatized substances opens the door to use of other drugs. The old idea of “gateway drugs” as a major concern has been challenged more recently as not so serious after all. For example, some newer thinking is that experimental substance use can be a normal rite of passage especially among young people.
- But laissez-faire attitudes about general experimentation with substances might no longer apply so widely, and might now depend on the specific substance of concern.
- For example, I ask myself “Today’s potencies are a gateway to what – an early death?”
“Chemical hooks” is a newer name for the drug effects like euphoria and craving that increase as potency increases. The idea of “chemical hooks” has been widely challenged more recently. And it has nearly been replaced with an alternative explanation of why people become addicted: Adverse Childhood Experiences.
- But failing to appropriately recognize dramatically higher potency might not properly factor in some relevant contributions of addiction-related morbidity and mortality being faced today.
- And I wonder, “Are ultra-potent formulations really not compelling in their impact?”
Given the commonly catastrophic harms (impacts) of even a single use of certain compounds, it seems to me that today Prevention, Harm Reduction, Peer Support, and Recovery Coaching should be components of one discipline.
And it seems to me that the aims of each of these individually are not diametrically opposed, but are in fact shared:
- Increased quality of life
- Decreased harmful impacts of use
Does Prevention become irrelevant during addiction treatment or during recovery from addiction illness? No – prevention remains relevant.
Prevention efforts that happen during one’s active addiction illness could prevent the initial use of a new and dangerous substance, as well as the related impacts (e.g. opioids and death from a single one-time use, or cigarettes and death after years of slow demise). Does Prevention become irrelevant during active addiction illness? No – prevention remains relevant even then.
Prevention, Adults, and Older Adults
Generally, our previous model of prevention made efforts before initial use, was aimed at the young, and was certainly undertaken before any disordered substance use. But that Prevention model also generally missed opportunities with those experiencing an onset of use late in life, those retiring, or those that lost a spouse.
Recent changes in society (at least within the USA) add stressors to our social system and to us individually. Our collective and individual adaptations may work for or against our interests in the short term or longer term. Compounding the pressure is the SARS-CoV-2 pandemic.
Consider the importance of “Prevention” in that context and in the face of these findings6:
- Early retirement is risk factor for mortality
- Prolonged working life may provide survival benefits
- 1 year older at retirement = 11% lower risk of all-cause mortality independent of sociodemographic data, lifestyle, and health confounds
- Unhealthy retirees have lower all-cause mortality when retiring later.
Looking Forward
Newer models of SUD services have emphasized implementation of:
- harm reduction strategies,
- innovation of new harm reduction approaches,
- harm reduction strategies as an outreach and stabilization method,
and may be followed by formal treatment. But those efforts have generally missed opportunities related to tertiary prevention and those late in the course of illness.
Historically, across the USA, provider organizations helping those with serious and complex addiction illness have arisen from motivated non-professional helpers, rather than formal systems of clinical care. That has resulted in both strengths and weaknesses within systems of care.
More recent empirical examinations of older methods like the DARE program and the still widespread clinical practice of ignoring cigarette smoking during addiction treatment have demonstrated opportunities to improve.
I suspect the current stressors in our society and in our systems of care for substance use disorders will result in problems that indirectly help bring about an improved model that will include:
- Training and service provision that is more like dentistry (a whole and unified model, comprised of wellness, prevention, and treatment with all methods available, across the lifespan)
- Harm reduction and Prevention as twin methods both available in all services and levels of care.
- Less opportunity for helpers to inaccurately project their own personal or professional experience as the proper method or path for the person served.
Some Personal Reflections
Having worked in a long-term (9-12 month) residential program:
- prior to and during that program’s initial shift to gender-specific care for women, and
- during its initial specialization to serving pregnant, post-partum, and parenting women (including having infants and children up to age 4 living with their mothers during treatment) – and
- doing the work of those specializations for the following 17 years,
I have a certain level of awareness and sensitivity to the topics in this essay as they pertain to prevention and the lifespan – to say nothing of the new problems caused by unprecedented potencies.
Later in those 17 years I undertook some personal study in developmental neuropsychology7, 8. In doing so I came to appreciate the basic biology related to cells differentiating after conception into neurons, and those neurons later migrating, developing and sub-specializing within the human physical system.
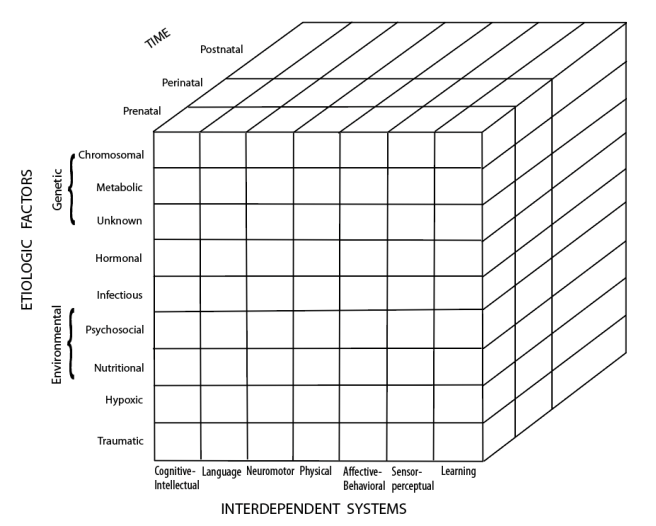
The diagram below, called the “Developmental Disabilities Cube”8, summarizes the major relevant domains of neuropsychological development and function. Think about today’s ultra-high substance potencies and the possibility of prevention across the lifespan as you consider this diagram.
Developmental Disabilities Cube
For me, witnessing over 17 years of:
- pregnant, post-partum, parenting women entering residential addiction treatment (many bringing an infant or toddler in to live with them during treatment);
- women returning to the program from the hospital after delivery of their infant;
- infants then entering the building to live with their mother during her stay;
- the results of developmental and functional assessments with those infants shortly following their birth and throughout the mother’s stay;
- the results of the targeted developmental interventions we conducted where some lags might have been present;
and outpatient methadone maintenance for 19 years
gives me a certain kind and range of clinical experience from which I can draw memories of patient narrative and case data. Those experiences help me have first-hand examples of various interactions between the causal factors and interdependent systems pictured in that diagram.
I have two suggestions to modify the diagram for our work:
- add clinical substance-related prevention techniques as an etiologic (protective) factor on the left-side vertical list;
- add segments of the entire life span (infant, child, adolescent, adult development and aging) after the “postnatal” phase at the back of the diagram.
References
1 https://recoveryreview.blog/2019/10/24/harms-of-use-a-list-of-references/
2 Nutt, D., King, L. A., Saulsbury, W. & Blakemore, C. (2007). Development of a Rational Scale to Assess the Harm of Drugs of Potential Misuse. Lancet. 369: 1047-1053.
3 Mazea, I. & Nestler, E. J. (2011). The Epigenetic Landscape of Addiction. Annals of the New York Academy of Sciences. 1216:99–113. doi:10.1111/j.1749-6632.2010.05893.x
4Verhulst, B., Neale, M. C. & Kendler, K. S. (2015). The Heritability of Alcohol Use Disorders: a meta-analysis of twin and adoption studies. Psychological Medicine. 45(5):1061–1072. doi:10.1017/S0033291714002165
5 Hall, O. T., Hall, O. E., McGrath, R. P., & Haile, Z. T. (2019). Years of Life Lost Due to Opioid Overdose in Ohio: Temporal and Geographic Patterns of Excess Mortality. Journal of Addiction Medicine. Open.
6Wu, C; Odden, MC; Fisher, GG & Stawski, RS. (2016). Association of Retirement Age With Mortality: A population-based longitudinal study among older adults in the USA. Journal of Epidemiology and Community Health. doi:10.1136/jech-2015-207097
7 Horton Jr., A. M., Ed. (1990). Neuropsychology Across the Life-Span. Springer Publishing Company: NY.
8 Spreen, O., Risser, A. & Edgell. (1995). Developmental Neuropsychology. Oxford University Press: NY.
Suggested Reading
Ciccarone, D. (2019). The Triple Wave Epidemic: Supply and demand drivers of the US opioid overdose crisis. International Journal of Drug Policy. doi.org/10.1016/j.drugpo.2019.01.010
Lewera, D., Tweede, E. J., Aldridgea, R. W. & Morley, K. I. (2019). Causes of Hospital Admission and Mortality Among 6683 People Who Use Heroin: A cohort study comparing relative and absolute risks. Drug and Alcohol Dependence. 204. 107525. doi.org/10.1016/j.drugalcdep.2019.06.027
Acknowledgement
Thanks to B. Schlosser for the artwork preparation of this representation of the Developmental Disabilities Cube.

Since 2016, Lorie Hammerstrom has been the lead onsite trainer for SMART. She also facilitates the teen and young adult meetings. Her passion for working with teens and young adults is evident in the hundreds of people she has helped in their recovery journey.

Rae Grady is an onsite trainer and Family & Friends facilitator, who has been with SMART since 2019. Her prior experience working with adolescents as a guidance counselor and crisis coordinator has given her the tools and empathy to support the those in need.
In this podcast, they talk about:
- Lorie’s need to find life goals beyond drugs and alcohol in high school and how it shaped her future
- Rae’s career working with adolescents and finding SMART as a resource
- How Lorie found SMART and why the tools were crucial in her life
- SMART’s principles are things kids can grab onto
- Why the school approach makes the teens more comfortable in meetings
- Lorie and Rae’s experiences with their own children’s struggles
- Why it’s important that teens learn to communicate
- The skills that trainers and facilitators need to work with teens and young adults
- The value in creating relationships with people
- Using music as a way to connect and relate to recovery
- Planting the seeds for recovery
- A mistake isn’t a failure, but an opportunity to learn
- The parents’ need to understand the recovery process
Additional resources:
Click here to find all of SMART Recovery’s podcasts
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @ 800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!
This essay was originally published by STAT on August 3, 2021.
Our understanding of substance use disorders as chronic but treatable health conditions has come a long way since the dark days when they were thought of as character flaws — or worse. Yet our societal norms surrounding drug use and addiction continue to be informed by unfounded myths and misconceptions.
Among the most harmful of these is the scientifically unfounded belief that compulsive drug-taking by individuals with addiction reflects ongoing deliberate antisocial or deviant choices. This belief contributes to the continued criminalization of drug use and addiction.
While attitudes around drug use, particularly use of substances like cannabis, have significantly changed in recent decades, the use and possession of most drugs continue to be penalized. Punitive policies around drugs mark people who use them as criminals, and so contribute to the overwhelming stigma against people contending with an often-debilitating and sometimes fatal disorder — and even against the medical treatments that can effectively address it.
Stigma has major negative impacts on health and well-being, which helps explain why only 18% of people with drug use disorders receive treatment for their addiction. Stigma impedes access to care and reduces the quality of care individuals receive. People with addiction, especially those who inject drugs, are often distrusted when presenting for care in emergency departments or when visiting other providers. They are often treated in a demeaning and dehumanizing way. And physicians holding stigmatizing attitudes may not provide adequate evidence-based care for patients with addiction.
A recent national survey of primary care physicians found that although most believe that opioid use disorder is a treatable medical condition, most also expressed similar stigmatizing views toward people with opioid use disorder that are held by the wider population. More stigmatizing attitudes among primary care physicians were correlated with lower use of medication in treatment of opioid use disorder and lower support for policies designed to increase access to those medications.
The perception of stigma by people with substance use disorders may cause them to avoid or delay engaging with health care or to conceal their drug use when interacting with health care professionals. Even when care is confidential, residential treatment or daily visits to receive treatment, particularly in close-knit communities, can be noticed and trigger judgment. According to the National Survey of Drug Use and Health, fear of negative opinions by neighbors or people in their community is one of the reasons people who know they need treatment for a substance use disorder avoid seeking it.
Fear of possible criminal consequences for drug use can shape people's health decision-making in many potentially deleterious ways. Substance use may be an important fact to consider in a routine medical visit, so its concealment can lead a physician to overlook major factors in a patient's health. In some states, pregnant people with substance use disorders risk being charged with child abuse or otherwise losing their parental rights if their child shows evidence of prenatal drug exposure or is born with neonatal abstinence syndrome. Fear of such consequences of substance use may cause individuals to avoid much-needed prenatal care, treatment, and other services.
The stigma against addiction extends to those who provide care for the condition and to the medications and harm-reduction measures that are used to address it. For example, methadone and buprenorphine are highly effective at helping people recover from opioid use disorders, but lingering prejudice that conflates taking medication with the use of harmful substances is one factor that prevents people from being treated with these medications.
Although treatment for addiction is becoming more integrated into medicine, it has faced major challenges on many fronts and requires overcoming health care providers’ attitudinal barriers as well as hurdles arising in part from confidentiality protection laws that may limit gathering and sharing data on patients' use of illicit substances. When doctors don’t ask about patients' drug use, they may miss information that is important to their care. Stigma also contributes to insurers setting restrictive limits on what they will cover for medications to treat substance use disorders.
Many people intersect with the criminal justice system as a direct or indirect result of their substance use disorders, and the experience may worsen their addiction and their physical and mental health. Although roughly half of people in prison have a substance use disorder, few receive treatment for it. People with untreated opioid use disorder are highly likely to return to drug use upon release, all too often with fatal consequences because of lost tolerance to the drug while in prison. Imprisonment itself not only increases the likelihood of dying prematurely but also negatively impacts mental health and social adjustment via the stigma of having been incarcerated. And it has radiating effects: Incarceration of a parent increases their children's risk of drug use, for example.
Research has consistently shown that when people interact with members of a stigmatized group and hear their stories directly, it has a powerful destigmatizing effect, more than simply educating the public about the science underlying a condition. But while a growing number of people in recovery are speaking openly about their past use and their current struggles to keep sober, people who use drugs actively — either because of an untreated addiction or during a period of relapse or even simply as a matter of personal choice outside the context of a use disorder — are not free to do so without fear of legal consequences.
The silence of people living with active drug use disorders due to the stigma associated with their condition means the wider public has no opportunity to hear from them and no opportunity to revise their prejudices, such as the belief that addiction is a moral failing or a form of deviance.
An effective public health response to substance use and substance use disorders must consider the policy landscape of criminalizing substance use, which constitutes a major socially sanctioned form of stigma. In addition to research already underway on stigma and stigma reduction at the National Institutes of Health, research on the positive and possible negative outcomes associated with alternative policy models that move to prioritize treatment over punishment are also urgently needed, as such models could remove a major linchpin of the stigma around drug use and addiction and improve the health of millions of Americans.
Nora D. Volkow is a psychiatrist, scientist, and director of the National Institute on Drug Abuse, which is part of the National Institutes of Health.

A while back, David Best and Dan Lubman published an article called ‘The Recovery Paradigm: A Model of Hope and Change for Alcohol and Drug Addiction’. I had reason to read it again this week and found much to encourage me in it. Here are some key messages from the piece with my comments in italics.
Recovery trajectories
in 2005, Dennis et al published longitudinal data from a sample recruited from a public treatment program in the United States suggesting that the average time from substance initiation to stable recovery is around 27 years.
We need long term supports for individuals. We need new ways to try to accelerate recovery while keeping people as safe as possible.
According to a review of international evidence conducted for the Centre for Substance Abuse Treatment ‘epidemiologic studies show that, on average, 58% of individuals with chronic substance dependence achieve sustained recovery’, although rates varied from 30–72%. however, as Warner argued, for mental health, this may not mean full remission. Rather, it may involve transcending their symptoms to lead a meaningful and fulfilling life, including making a valuable contribution to family, community and society.
Recovery is a reality and has knock-on effects beyond the individual.
Quality of life
In the UK, Hibbert and Best interviewed former alcoholics who had been abstinent for at least year. not only was there clear evidence of ongoing recovery growth, but those who were more than 5 years sober and in active recovery had better social quality of life scores than the general public.
Recovery improves quality of life.
In a follow up study in Glasgow of 205 former alcoholics and heroin addicts in recovery, the strongest predictors of higher life quality were engaging in more activities (volunteering, education and training, work and family) and more time spent with other people in recovery.
To improve quality of life in those seeking recovery, encourage involvement in structured activity in the community and connect them to other recovering people.
People matter
One of the most important things we know about recovery is that other people matter. the resolution of severe alcohol and other drug problems is mediated by processes of social and cultural support. Both general and abstinence specific social support influence recovery outcomes, but abstinence specific support appears to be most critical to long term recovery.
People need people to recover. Abstinence-specific support is important. (Though abstinence is not a prerequisite for recovery).
In a randomised trial of alcoholics completing residential detoxification, participants underwent either ‘standard case management’ or ‘network support’ – with the aim of the latter being to add at least one sober person to the social network of the detoxed drinker. Relapse rates in the network support condition were 27% lower than in the standard treatment condition, emphasising the key role of peer support in enabling long term recovery, and the core underlying principle of ‘social contagion’.
Peer to peer connection has a powerful influence on outcomes and reduces relapse rates. Recovery is infectious.
So does harm reduction
As addiction careers typically exceed a quarter of a century, a range of interventions will be required at different times. it is crucial to support and engage those with long term alcohol and other drug problems until they are ready to make lasting changes. this includes offering harm reduction approaches.
Harm reduction is key to supporting people on recovery journeys and should be a fundamental offer in services.
Professionals can help
Health professionals can instil hope that recovery can occur and should be mindful that their relationship can be a critical ‘turning point’ in the patient’s recovery journey, acting as a ‘bridge’ to groups and individuals who successfully model recovery, and involving family members.
Professionals can support individuals to change direction and to connect them to mutual aid and other community recovery resources (e.g. Lived experience recovery organisations [LEROs]).
Recovery rights are civil rights
We have learnt in recent years that recovery does not happen in isolation and that recovery can have the strength of a social movement akin to the civil rights movement.
Still happening, though my observation is that it is still at the ‘storming’ phase with too many factions and frictions, albeit achieving progress overall.
Summing up
Although addiction is a chronic relapsing disorder most people recover, with flow-on benefits to both individuals and communities. Within the mental health field, adoption of a recovery model can bring about significant benefits for individuals and families, can inspire hope in communities and is a cost-effective approach to delivering interventions. This approach readily lends itself to the treatment of addiction
Continue the discussion: @DocDavidM
Best DW, Lubman DI. The recovery paradigm – a model of hope and change for alcohol and drug addiction. Aust Fam Physician. 2012 Aug;41(8):593-7. PMID: 23145400.
Photo credit: gustavfrazao under license

Let’s say I cannot bowl very well. I have a bowling problem. My father loved bowling and was usually good at it, but he was also plagued with times where he was not very good; he was very hard on himself during those times. In fact, every time I try to bowl, I suck at it. Furthermore, like my father, I am very hard on myself about this fact. For whatever reason, I desperately need to become a better bowler.
I ask myself, “What would I do if I were given the choice of where to set up bowling pins, anywhere in the lane, in any configuration I wanted?”
To answer this, I would first identify how the official configuration does not match my bowling style (linear, rolled between squatting legs, granny style). Those fancy pro bowlers with their wrist guards and curving balls- not for me. The second part is the length; the lane is a bit long for my style. Of course, I still want to be rigorous, so I think a lane about half as long is probably best. So, halfway down at the mid lane, I set up my pins, knowing that my style consistently produces a straight bowling ball that rarely deviates beyond six inches of center and rolls at about half speed.
I want to be scientific, so I throw several regular games of “old bowling,” recording the score, then throw the same amount of games under this new configuration, “new bowling.”
Low and behold, my new method consistently and statistically produces much better scores than the old regime. This new method yields twice as many pins knocked down (PND).
My new method goes so well that I start writing all about it. I travel to bowling alleys, give presentations, lessons, demonstrations. I find niches for New Bowling (like kids bowling), I publish lengthy books on matching the best pin arrangement for your throwing style. I become famous, a “maverick,” an outspoken critic of the ineffective “old way” of bowling.
What is lost? Well, for one, the entire point of the game.
The game’s goal is not to just effectively knock down pins- although, from an outsider’s perspective, that is what bowling may objectively appear to be.
Second, as quaint as it may sound, the tradition, art, history, and meaning of bowling are lost. However, I do not know or care about that history. I just want to knock down pins effectively.
I do not even talk to my fellow bowlers at all. When they point out I may be “bowling wrong,” I fling their accusations back at them, label them “bigots, hypocrites.” I dig up research on wrist injuries from old bowling; I write about how it takes years for people to learn the old way, how scores for ordinary people are typically low, ESPECIALLY the FIRST TIME they play.
In a Tweet, I pronounce, “How do you expect people to have the confidence to keep learning to bowl, if, in their first game, the scores are almost ALWAYS LOW and people feel ashamed?”
I publicly question whether bowling is even a “sport”- I mess around with language. I say to people, “This so called ‘sport,’ is for dominant classes of the privileged, who have the luxury, time, and access of training. Not everyone can train to be a good bowler. Not everyone wants to be a bowler, some just want to knock down pins. I want to see bowling pins set up in such a way so as to be able to be knocked down by anyone.”
See how egalitarian I am? See how I bring justice to the injustice of this so-called “sport”?
I even write a personal book about how my abusive dad tried to teach me bowling, how this gave me anxiety, how this anxiety crippled my ability to learn the skills I needed to be successful in the old bowling style. I throw in graphs, statistics, studies on performance anxiety.
Everyone is sympathetic. The book is a hit. I Tweet, “I survived shamed-based bowling and THAT is WHY, I am pushing for a better way.”
Headlines thus declare, “New Bowling is Evidence-Based Bowling, and it doesn’t carry the shame of the old style.”
Do you want to knock down pins? Here is how to do it BEST, and in a way that is not only accessible to all but sheds the “old way,” the “Al Bundy way” of “shame-based bowling.”
And those that still bowl in the old way? That is fine, but ALL bowling alleys should have several lanes DEDICATED to New Bowling. If not, you are discriminating against people based on their bowling style, skill, and what they want. Moreover, this is the EXACT problem with “Shame-based Bowling.”
Well, demand for New Bowling goes up. Bowling alley owners who do not adapt are accused of being “anti-scientific,” of relying upon “ghosts of the past and bowling folk tradition.”
So what happens? Well, a whole new movement and push for New Bowling emerge. Policymakers get involved, grants to study and compare pins knocked down (PND) are made available, bowling sponsors change their tune. A whole system of money, business, and science that once relied on the holistic vision of bowling as a sport now becomes a self-referential system that claims New Bowling to be superior, more just, and a better way to spend bowling money. A whole system of money and science becomes the rationalization apparatus of New Bowling. The Jury is in, the evidence is clear, New Bowling is JUST BETTER.
I tweet, “Al BUNDY BOWLING KILLS SELF-ESTEEM,” and it gets millions of retweets.
Long-time bowling instructors, and their bowling clinics, become pariahs. When they speak about the holistic benefits of learning to bowl, people shout over them, “Yeah, but HOW MANY PINS ARE THEY REALLY KNOCKING DOWN?” or “How many EGOS have been murdered by the shame created by these so-called “bowling clinics?”
Billing for bowling clinic hours becomes dominated by how many pins the students can knock down per session (PNDPS). This measure becomes the standard rubric for all bowling clinics. No sufficient PNDPS number? No compensation.
Along the way, no one is allowed to question the whole picture. No one asks if the number of pins knocked down should be the focus of the science of bowling. No one reads the fine print.
In the search to find a better way to knock pins down for people who lacked bowling skills, I missed the entire point of learning the craft of competitive skills that, at times, can transcend all other life challenges.
A perfect game- rare, yes, but when it happens, everything else becomes less important- car trouble, bills, the daily grind. For a small moment, none of that matters when there is a perfect game. The discipline the bowler learns from not bowling a perfect game also has its rewards. By practicing every day, the bowler gets better. They see themselves as a bowler. They are proud of themselves, even on days where they do not bowl a perfect game.
The whole point of the sport is dedication, honoring the traditional values of competition, practices, and daily effort. The point is to join in an activity with others, laugh, smile, have fun. It is about learning about oneself. Bowling is not valuable because of the pins knocked down each day. It is valuable because those dedicated to bowling are changed in seeking to do so each day. What they learn at the alley becomes a metaphor for living. The friends they make at the alley are their support networks in real life. The point is not knocking down pins. The point is to become a better person by honing the craft- by seeking to do so through practice, community, and effort.
Yet, The Journal of Bowling Science declares: “New Bowling is, in fact, BETTER”*
(*at increasing the number of pins knocked down).
By measuring the wrong thing, I have entirely missed the potential of what bowling can do for the bowler. By negating the qualitative input of long-time bowlers, bowling instructors, new bowlers, league reps, and alley owners, I lose sight of the motivations, connections, memories, feelings, and pain of those who actually know what bowling is about. I lose sight of the aggregate truth: the truth of what it means to bowl and to be a bowler.
Instead, I insist that such research is “just unscientific” and not generalizable. After all, facts do not care about feelings. Besides, such research is not “cost-effective.” I get my fellow statisticians to weigh in, they agree. It simply is not feasible to account for those kinds of qualitative effects that are so individualized. What it means to bowl and be a bowler is not an observable fact. All science can and should measure is PND, and therefore, the old bowling ways are terrible at producing outcomes. It is better if science sticks to observable facts.
By measuring the wrong thing, I have not only missed the point of what bowling does for the bowler, but I have also negated the discussion of the benefits of learning to bowl. While at the same time creating a whole system that prevents me from ever truly and scientifically coming to understand what it means to bowl and to be a bowler. Instead of Bowling Science communicating ways that bowling instructors can teach better old-style bowling or exploring the joy of bowling, the science of technique- Bowling Science becomes the art of bean-counting, the journal of standards for PND counting.
Instead of the joy of watching a new bowler learning new skills, instead of teaching about discipline, fun, dedication, fair play, and the gifts of learning to bowl (no matter how many pins fall), the bowling instructor is reduced to manualized technical instruction and LOTS of PND counting and billing for those PNDPS.
If I want to measure bowling “outcomes,” I cannot do so by simply quantifying the number of knocked-down pins, no matter how observable this may be. No matter how instinctively rational and scientific the counting of pins knocked down (PND) may seem. No matter how logically appealing it may be, this is the absolutely incorrect way to measure what bowling does for the bowler.
Special Thanks to Brian Coon whose email inspired this post.

Alexa Johnson is a friend who is early in her career and reached out for my thoughts on some important questions she had been contemplating. She shared a written reflection on the issues involved and I encouraged her to turn it into a post. I admire her combination of conviction and willingness to keep asking questions of herself and others, tolerate dissonance, and make adjustments. Hope you enjoy!
I work with people seeking recovery and we have a saying that goes, “We never know who’s going to walk through our front door.” When I first heard that, to me–a brand new “normie” with zero knowledge on addiction or recovery–that meant people from all walks of life like people with felonies, sex workers, and doctors. What hadn’t occurred to me was that it also included racists.
Working at this treatment center, we serve a majority of white clients. As a Black and Latina woman and the only brown counselor working in the detox facility for a while, I quickly became the person that BIPOC clients confided in when situations surrounding race came up. I made it my duty to call out and hold everyone accountable that put BIPOC clients in harm’s way- staff and clients alike. I made sure that no racist stone went unturned. I fiercely and consistently advocated to take clients to more Narcotics Anonymous meetings because they are typically more representative of the Black community, and also outreach efforts to bring in more people of color to create and re-establish a culture of recovery that everyone feels safe in.
…this could be a dialectic. This man could be very racist and still deserve to live a life free of the suffering that addiction brings.
Over the course of my two and a half years here, there were several clients that I believed should no longer be able to receive treatment with us. One client in particular was involved in a harmful situation, and although it was brought to the appropriate person’s attention- nothing came of it. I was pissed, the Black client was scarred, and the white client walked away unscathed.
Two years, multiple situations, and a 6-hour anti-racism training later, that same white client returned to us for a level of care assessment. Confused on what to recommend due to this client’s past acts of racism, his therapist consulted another therapist and he came to the conclusion that he should have the opportunity to return and address his behavior in treatment. I was confused and angry. How could this even be considered? This client can absolutely not come back to our services. A couple months later, I revisited the idea- could that therapist have been right?
I’m blessed to work at an organization that hires people in recovery. Over my few years with them, the amount of knowledge I’ve received has been invaluable. So, why didn’t I believe that this therapist (who is in long-term recovery and an MSW graduate) knew what he was talking about? To be honest, it was very difficult for me to wrap my head around the idea that this could be a dialectic. This man could be very racist and still deserve to live a life free of the suffering that addiction brings. We are not in the business of turning bad people good, but helping sick people get well.
As a woman of color, I struggle daily with this idea. In no way, shape, or form do I condone racist, homophobic, or sexist actions. Advocating that the BIPOC community, my community, deserves equal treatment (in regards to recovery as well as respect), reminding folks that racism is a sobriety threatening issue, and trying to create safe spaces- while also advocating that even racist people deserve treatment and focusing on principles over personalities is… confusing to say the least.
We call addiction a disease, I would call racism the same. Meaning it’s chronic, progressive, often fatal, as well as cunning and baffling. Outcomes of conversation or self-reflection such as an urge to be anti-racist or having the courage to change are desired, however, not always achieved. As a professional in this field, sharing the burden and walking alongside an individual as they unpack a lifetime’s worth of biases and trauma becomes the primary purpose of our work. There’s an amount of labor that goes into learning about recovery and I believe the same goes for racism. With this being said, recovery is possible.
I think it’s imperative that we as addiction professionals and aspiring recovery allies keep in mind the harm of turning away or kicking out individuals who have been racist and also weighing the harm of racism for our clients of color. Choosing one over the other feels negligent and life-threatening for our clients and patients. We must consistently ask ourselves, what can I do to be less performative and more restorative?
A blurb from the Alcoholics Anonymous Big Book that keeps me looking forward is,
Shakespeare said, “All the world’s a stage, and all the men and women merely players.” He forgot to mention that I was the chief critic. I was always able to see the flaw in every person, every situation. And I was always glad to point it out, because I knew you wanted perfection, just as I did. A.A. and acceptance have taught me that there is a bit of good in the worst of us and a bit of bad in the best of us; that we are all children of God and we each have a right to be here.
AA Big Book p 417

Forward: I have known Bev Haberle and her work for a long time. We are both from Eastern Pennsylvania and our paths crossed regularly over the years. I brought her staff into the residential facility I ran in the early 2000s to meet and engage our alumni. Bev served for many years as the Executive Director at The Council of Southeast Pennsylvania, Inc. a program providing information, education, prevention, treatment, and recovery services throughout the five counties of Southeastern PA. Pennsylvania Recovery Organization Achieving Community Together (PRO-ACT) was one of the projects that rose out of The Council to mobilize the recovery community. The PRO-ACT project and the 501c3 statewide recovery community organization I now run, The Pennsylvania Recovery Organizations – Alliance (PRO-A) were started around the same time and have always been confused with each other. We were both in the first cohort of the Recovery Community Service Program (RCSP) grants and the organizations became aware of each other in the late 90s as these initial competitive grants were awarded. Two wonderful recovery community organizations, seemingly forever confused.
One of the stories that I heard Bev tell over the years about her own journey into recovery 50 years ago in 1971. Bev graciously gave her permission to share it as part of this interview. As a young woman, she nearly had a prefrontal lobotomy performed on her as this was a procedure that was used on persons with alcoholism in that era. It was harm disguised as help. This type of brain surgery can radically change a persons personality and cognition. A person in recovery learned about her plight through her church and reached out to her, offered her hope and helped her get into recovery. She took another path as a result and is forever grateful that tragedy was averted, tremendous things resulted. When she shared her story with Bill White she said that experience became the motivating factor for her work to assure dissemination of accurate information and advocacy for research based quality treatment.
Over the years before her retirement, Bev and PRO-ACT would join other early recovery community organizations like The RASE Project and The Message Carriers of Western PA with PRO-A to advocate for issues of common concern for the recovery community of Pennsylvania. As I conducted this interview, we also had a few side conversations about how people have come together to help others experiencing addiction over the long arc of American history. A number of these conversations went back to Marty Mann, who was the first woman in Alcoholics Anonymous and who also started the National Council on Alcoholism and Drug Dependence (NCADD). Marty probably did more to raise awareness and support for persons with alcoholism than her more celebrated male counterparts Dr Bob and Bill Wilson. It is a reoccurring theme through these interviews that knowledge of our own history and adhering to recovery values underpinned the effort.
Bev Haberle served for over 40 years as the Executive Director of The Council of Southeast Pennsylvania, Inc., a non-profit recovery community organization that provides prevention, intervention, education, advocacy, and addiction recovery solutions. For the last 22 years, Bev served as the Project Director for Pennsylvania Recovery Organization-Achieving Community Together (PRO-ACT), a grassroots advocacy initiative that promotes the rights of, and ensures opportunities, for those suffering from substance use disorders, members of the recovery community, and their family members.
Bev holds a Master’s degree in Human Services, is a Licensed Professional Counselor, a Certified Advanced Alcohol and Drugs Counselor, and a Certified Intervention Professional. She was the co-founder of the National Intervention Network. Bev has served on a number of local, state and national Boards, Coalitions and Committees. In the past, she had been a member of the Board of Directors for the National Council on Alcoholism and Drug Dependence, Inc., Vice Chairwoman for the National Board of Directors for Faces & Voices of Recovery and also Co-Chair of Philadelphia’s Office of Addiction Services Advisory Board, to name a few. She is a person in long-term recovery (50 years) and a person of faith. She is an ordained Elder of her Church. She has been an active advocate on behalf of those with substance use disorders, their families and the community at large for over 40 years. In 2018, Faces & Voices of Recovery honored her service to the recovery community with the Distinguished Lifetime Achievement Award at their annual America Honors Recovery awards dinner.
- Who are you and what brought you to Saint Paul at that time?
The story of how I ended up in Saint Paul at the 2001 Recovery Summit started with the formation of PRO-ACT a few years prior to that, in the mid-1990s. The project was developed because of the growing recognition at that time that substance use treatment was changing. Treatment was not providing the kinds of community support people needed. The kinds of things that many of us had received through it a generation before. Treatment was becoming detached from the recovery community. We started to mobilize people in the region. Around that time, the RCSP grants came out and we got one. It was not until we got to DC for the initial grant meetings that I became aware that there was a second grant recipient in PA, PRO-A.
That SAMHSA RCSP grant and the coming together of the recipients was foundational to what occurred. We met and worked together for several years to strengthen recovery efforts prior to the summit in 2001. There were 18 of us, and the way that the grant administrators worked with us was also an important facet of how it came together. Cathy Nugent was our grant officer, and June Gertig and Rick Sampson from SAMHSA were also involved. They helped facilitate our connections and validated the principle that people in recovery were the experts in recovery. They listened to us. It was incredibly validating in ways that I don’t think even occurred to us at the time.
We stated to bring people together to advocate for long term recovery using whatever pathway got them there, including MAT. It was an interesting time. I initially thought that when we started to bring people together that it would be people in long term recovery who would stand up, but it was not. When we would talk with people in long term recovery, they did not have a sense there was anything wrong. They did not see the stigma or the disparate treatment. It was like they got their lives back and were content golfing and having a good life. It was not what we were seeing on the ground when we began working with people in early recovery. It was the family members of people still suffering, people in early recovery, people in reentry from the criminal justice system and people living in recovery housing. They were the people who showed up. The kind of connection and the development of recovery community were exactly what they wanted. People really began to mobilize around the idea that we needed to be more open about recovery and start sharing our stories about recovery.
We formed strong connections within the RCSP grantee cohort and we were having similar conversations with community members across the nation. There are so many complex dynamics that make recovery a highly individualized experience. Things like gender, race, economic status, sexual identity become even more complex in the context of individual values, and anonymity. We began to really recognize the power our stories to share hope and the benefits of recovery. Everything we did was grounded in recovery values. Humility, honesty, and integrity were things we worked very hard to center our work on. Bill White was very involved with us. He had just published his book; Slaying the Dragon and we became aware of the rich history that had preceded us. We shared different ways of looking at recovery and people like Don Coyhis introduced us to Native American rituals of recovery. Tom Hill highlighted his experiences through the gay rights movement and the need to stand up and not being silent as our people continued to die. Many of us started to feel free in a way that had not occurred in our lives prior to us all coming together. We knew it was powerful.
While we thought of ourselves as the first as we were doing this work, we also become keenly aware of how many generations of recovery community who came before us. That fact – that so many had come before us was deeply humbling. We were conscious that what we were building was fragile. Our own history shows us this truth. Unchecked ego, the quest for power and self-serving agendas would derail our efforts if we did not pay attention and keep our agenda focused on our common purpose.
I am not sure what we all expected when we got to Saint Paul. I know we had reached consensus that inclusion of many pathways of recovery was important to us. This was a radical notion back then, as was the idea that we should step out of anonymity and share who and what we were as people in recovery. I think we were hoping that we would find validation and acceptance of what we had all been working on, rather than the deficit focus on addiction that blocked out all of the benefit of a recovery focus that we wanted to start talking about.
- Is there a particular moment or memory that stands out to you from that summit?
I don’t think we realized what Saint Paul was about until we got there. We went because our grant officers encouraged us to do so. I am glad they did. As an aside, when I first got into recovery, I did not feel like I experienced discrimination because I hid behind my Anonymity. I recall feeling shame and guilt for the first time several years later when I was sitting in a classroom learning about alcoholism. The professor started talking about “those people.” I realized she was talking about people like me. That was a real awakening. It is also true that I served as Executive Director of a substance use prevention and treatment organization for 13 years prior to the summit, and I don’t think I ever once publicly acknowledged my recovery status. Most of us who served within the substance use care system hid our recovery up until that time. Talking openly about recovery just wasn’t done.
When I was sitting in that room with all of us from across the nation, I saw elected officials, leaders of treatment organizations and others stand up for the first time and openly talk about recovery. I was with my people. I was overcome with pride and hope, not for myself but for all the people who needed hope and needed help. The potential of what we could do was clear to all of us. I had been a little concerned up until that moment that this was going to be like all the addiction focused conferences I had ever attended. Deficit focused. Instead, they started to talk about recovery, and I realized that they get it – they knew that the pathway forward was to focus on hope and bringing our communities together for common purpose. It was a powerful moment for all of us.
- What did you see as the motivating factors that brought you all together for that historic summit twenty years ago?
I don’t think I can overstate the foundational work that we did through those SAMHSA RCSP grants. The work we did together was crucial. There was a collective momentum that started before the summit that became even more powerful after Saint Paul. As I mentioned before, I also think what Bill White was doing to document the rich history of recovery movements through his book Slaying the Dragon was very much in our thoughts. We knew what we were doing was important. We also knew that we had to be very careful. It was critical that we build our work on recovery values if what we wanted was to be sustained over time. We knew that how we did it mattered as much or even more than what we did. I hope this fact does not get lost in history. We realized that if we did not ground everything in our shared values that it would all eventually fail. It is an often-repeated dynamic in our own history we must stay vigilant about. What was true then and remains true today, is that unless we build everything on a foundation of shared recovery values, consensus building and mutual positive regard, it all will fall apart.
- How have we done in accomplishing those early goals?
We have accomplished a whole lot. I think that changing how we talk about recovery was one of the most important things we did. I remember one of our early trainings at PRO-ACT. We were educating people about how to talk about recovery. We emphasized recovery, not addiction. We would say “my name is Bev Haberle and I am a person in long term recovery and what that has meant in my life is….” We don’t label ourselves as alcoholics or addicts in public settings anymore, it sends the wrong message. I recall teaching that to a young woman and she started crying and she said how much better that felt. We were teaching people how to talk about the dignity and worth of recovery. It really resonated with the community.
I think we have also made some progress with philanthropic efforts. For so many decades we have had no benefactors. Even some of the wealthiest families in America who have seen the power of recovery to heal their own families and experienced the devastation of addiction would never consider supporting recovery as benefactors. Instead of supporting efforts that saved their own families, they added yet another hospital wing or a university library. Of course, this is because of stigma, but it is starting to change.
We are also seeing more awareness in political circles than we had in past times. When we first stated the Recovery Walks event in Philadelphia, we would send out invitations to elected officials and other than a few like Gene DiGirolamo, they just didn’t show up. That has sure changed as politicians have begun to realize we do vote and that we are a constituency of consequence. A few years back when we had 30,000 people show up for the walk, we had so many elected officials who wanted to be involved that we did not have time on the schedule to have them all talk on the stage. We acknowledged them by having them walk behind a banner that indicated they were elected officials who supported recovery. A real change in attitude about the need to support Recovery. I also see it with our recovery voters’ guide that Noni West had put together over the years. Our community wants to know where people running for public office stands on recovery. This is all progress we have made!
- What do you see our greatest successes to date are?
I think our efforts to elevate recovery into the conciseness of the general public has saved a lot of lives. We are seeing less stigma in some communities. Families are more likely to seek help earlier. There is a lot more awareness that there are many pathways to recovery. We have even made with strengthening efforts to treat addiction alongside of co-occurring mental health needs when both our present. This is all progress, all of it rising out of our collective effort to educate the public and raise awareness about recovery.
- What did we miss if anything looking back at those goals?
We really should have focused on a comprehensive research agenda to better understand long term recovery. The hard science that supports the work to get more people into recovery and to sustain recovery over the long term. We did not invest in research to the degree we should have. There were some early efforts, like the Life In Recovery study, but we did not focus enough of our energy on recovery research as we should have. We need hard science on recovery, had we focused there, we would be in better shape today. We need to understand how people access recovery and sustain it. We need to understand gender differences, racial and cultural differences and how we support diverse communities to obtain and sustain recovery.
We need to develop deeper insights into recovery capital and the myriad of pathways and supports people use. Such hard science would only benefit us, but we simply don’t have it. Nearly everything we have is on public treatment, almost nothing on recovery community or how varied our individual experiences are. I can tell you that as one of the few women who attended recovery fellowships in my community in the early 70s it was hard and we have different needs than men. We spoke earlier about Marty Mann, she blazed the trial for us, but we still don’t have a complete picture of the recovery needs of women in recovery. I don’t think we have a good scientific understanding of how varied recovery experiences are. We need that hard science to help us understand how to save more lives.
- What are you most concerned about in respect to the future?
History shows us very clearly that there is a pendulum that swings. We make forward progress and then we risk falling backwards. I am concerned that we might fall back too far and lose a lot of ground we worked very hard to gain. I think we need to have more community discussions about our foundational recovery values. I think for some reason elements of those values have been lost along the way. If we do not ground our work in values such as humility, honesty and integrity what we built will fail. It seems like people in recovery in our current era move too quickly into the role of expert. Not everyone has to be a professional. It probably would make sense to spend a lot more of our time focusing on strengthening common values of recovery and orienting people on why these values are critically important. We risk becoming over professionalized. This was never our intention. We always envisioned a broad volunteer effort as the base of the recovery movement.
I recall one of the Recovery Community Centers I was involved with and how much effort we put into building an authentic advisory group. People who served on this advisory group/Vision Team were charged with keeping us focused on the needs of the community and making sure everything we did was done with high ethical standards. They were charged with being Stewards of quality recovery support services that meet the needs of the local Community being served. There was a lot of open discussion about what we were doing and we worked hard to make sure we stayed true to our community mission. They often spotted things the rest of us missed. People coming into our centers with what on the face of it looked like beneficial things but who had hidden agendas or self-dealing schemes. As a leader, I knew we needed them as our anchor to our mission.
I watched over time what was put together decay and gradually move away from the needs of the community. Some Centers lost focus on process and ended up going through the motions without paying attention to the needs of the community. This is not an uncommon dynamic. The newer people did not understand why we put those things into place and the vital function they served. So they gradually stopped doing them. Things did not work as well as a result. It is a lesson to heed. We need broad and open community engagement. We must have servant leadership who listen more than they talk and who are willing to look at the hard things and listen to the difficult feedback in order to stay true to the authentic recovery community. Anything less will fail us. We need to focus on this.
- What would you say to future generations of recovery advocates about what we did and what to be cautious of / your wishes for them moving forward?
90 Meetings in 90 Days…It’s not just for newcomers!
By Caroline Tisdale, Fellowship Hall Counselor
If you’ve recently completed treatment, your counselor probably suggested you attend 90 meetings (AA or NA) in 90 days – and you probably wondered, “do I really need to go to a meeting every single day?” The answer is YES and here’s why:
- 90 for 90 is not just for newcomers. We encourage newcomers to go to 90 meetings in 90 days immediately following treatment because you need connection and the fellowship of a 12 Step Program – it also really helps with finding a sponsor.
- When you’ve done 90 meetings in 90 days – start over. Attending a meeting keeps you engaged in a constructive activity – if you’re not at work, or volunteering, or helping out your family, why aren’t you at a meeting?
- 90 for 90 is a great way to gain experience, strengthen your recovery, and keep the hope going strong through interactions with lots of people who have good experiences to share.
- 90 for 90 is a great way to recommit to your recovery when you find yourself feeling complacent. Maybe you’ve been in the program for a while, you’ve worked the 12 Steps, you’ve sponsored people, and you find yourself saying, “what else is here? What is my recovery about?” 90 for 90 can help.
- 90 for 90 can be a life-saver when something significant is happening in your life. The people in meetings have experience and will offer support to help you navigate life changes.
- 90 for 90 is for old timers too! Oldtimers go for the newcomers to share their story and help them get sober. If we want to stay sober and have a happy life, we are required to carry the message to other alcoholics and addicts. This is a fundamental tenant of the 12 Step Program. 90 for 90 is for everyone.

Caroline Tisdale (LCSW, LCAS, CSI, CCTP-II, RYT200) is a social worker by profession and this is her second career. She graduated in 2017 with a masters in social work from the Joint Master of Social Work Program between NC A&T State University and the University of North Carolina at Greensboro after having had a long career in public health working in HIV/STD prevention. She is passionate about working with people experiencing addiction and assisting them with their healing process and starting the road to becoming the people they truly are. She is a licensed clinical social worker, a licensed clinical addictions specialist, a clinical supervisor intern, a certificate complex trauma professional, and a registered yoga teacher at the 200 hour level.
About Fellowship Hall
Fellowship Hall is a 99-bed, private, not-for-profit alcohol and drug treatment center located on 120 tranquil acres in Greensboro, N.C. We provide treatment and evidence-based programs built upon the Twelve-Step model of recovery. We have been accredited by The Joint Commission since 1974 as a specialty hospital and are a member of the National Association of Addiction Treatment Providers. We are committed to providing exceptional, compassionate care to every individual we serve.

In Scotland we have the highest number of drug-related deaths in Europe, perhaps in the world. We had a shameful 1399 drug-related deaths in 2020. Our alcohol-related deaths are also alarming. A lot of effort and resource is going into tackling the issue which we hope will make a difference. There are calls for much more to be done. What else can we do though? What is missing? Could there be a non-medical, simple-to-implement intervention that would make a difference?
Getting plugged in
The concept I’m contemplating is simple and it’s not my idea. It’s this: healthy social networks (the people we connect with) are protective. Improving social networks brings gains in physical and mental health. People suffering with addiction frequently have damaged or unhealthy social networks. They are often dislocated and estranged or excluded from being active community members. Connecting them back into supportive networks is likely to be of benefit. As I say, there is existing evidence on this, though there are serious questions about how far it has penetrated into the practice of treatment providers or commissioners.
If we look at existing research, there’s no better place to start than examining the impact of social networks on longevity and wellbeing. In 2010, Julianne Holt-Lunstad and her colleagues undertook an impressive meta-analysis (massive review of the evidence available) to see how social relationships influenced mortality. They found a protective effect for those with stronger social relationships. In fact, for this group there was a 50% increased likelihood of survival. In medical terms, this is a very large effect – similar to stopping smoking. You want to live longer? Get lots of friends.
Mark Litt and his colleagues explored this concept in alcohol-dependent men and women in 2009. In a high-quality trial, they tested out linking individuals into new pro-abstinence networks vs. other established treatments and found that those who formed new connections (in mutual aid) did better than established treatments. A stunning finding was that:
the addition of just one abstinent person to a social network increased the probability of abstinence for the next year by 27%.
Litt found that drinkers’ social networks can be changed by a treatment that is specifically designed to do so, and that these changes contribute to improved drinking outcomes.
A recent Cochrane review of the impact of Alcoholics Anonymous and interventions to help people get connected to it scotched many of the myths that sceptics attach to mutual aid.
So how are we doing on this front?
If we could get this sort of impact from medication in alcohol treatment settings, we’d be very happy, and if you are like me, you’ll be thinking, ‘lets go for it!’ Yet when commissioners asked 250 addiction treatment service users in Edinburgh in 2010 how many of them had ever been to a mutual aid group, the answer was less than 1%.
This is pretty dismal. In 2010, we weren’t doing very well in the city of Edinburgh. My hope is that if this was repeated today, we’d see an improvement. But we don’t know, because nobody is measuring how effectively we are connecting our clients to community recovery supports like mutual aid and lived experience recovery organisations (LEROs). This suggests that we don’t rate this kind of intervention as being relevant to our fight against drug deaths.
Getting equipped for recovery
There are two papers recent papers that caught my eye which are relevant to this topic and are worth a read. I’m not going to analyse them here, but I will pick out some key points. In the first ‘Are members of mutual aid groups better equipped for addiction recovery?’, Thomas Martinelli and colleagues interviewed 367 people in recovery from drug addiction and looked at how membership of mutual aid groups related to things like social networks, recovery capital and commitment to sobriety.
They recruited the participants in Belgium, the Netherlands and the UK by a variety of methods including social media, newsletters, conferences, posters, flyers, magazines and by contacting prevention and treatment organisations. Participants self-identified as being in recovery for at least three months and completed a questionnaire.
Findings
Interestingly, 69% reported membership of mutual aid groups at some point. When lifetime mutual aid members were compared with non-mutual aid members, some differences appeared with significant benefits to the mutual aid group members. These were identified in things like: paid employment (64% vs. 45%); abstinence from drugs (94% vs. 75%) and abstinence from alcohol (81% vs. 52%).
For those who were using drugs or alcohol, using days and drinking days were 3 times higher in the non-mutual aid group. There were strong associations with improved social networks, increased recovery capital (and ability to sustain recovery) and commitment to recovery for mutual aid group members. Those who were current members of mutual aid groups consistently reported more resources than those who had been members in the past. The benefits were greatest for members of 12-step groups, but positive outcomes did extend to non 12-step groups too.
Bottom line?
the expanding evidence on the benefits of mutual aid group participation should justify further exploration of its inclusion into system-wide practice of addiction services and to encourage services to refer to mutual aid groups
Getting a dose of recovery
In the other paper which focuses on the negative issues associated with social networks – ‘Social network theory—an underutilized opportunity to align innovative methods with the demands of the opioid epidemic’, Christina Cutter and colleagues point out that demand for opioid use arising from social networks and environment is an important contributing factor to the current opioid crisis.
Previous research on behaviours shows cluster effects (e.g. around obesity, suggesting that if you want to lose weight, you should hang around with thin friends). They recommend that we explore the ‘social contagion model’, an approach which puts forward that behaviours develop through role modelling and spread as if they are infective.
Their argument focusses on the problem (how opiate addiction spreads) and they express how understanding and exploration of this could help develop new strategies. They powerfully describe the issue of ‘social networks of despair’ arising from overdoses and deaths, but they also shine a light, turning things around and presenting the opportunity for the social contagion model to operate as a catalyst for recovery. I often paraphrase this as ‘if you hang around people in recovery long enough, you are likely to catch a dose of it.’
Indeed, the authors give mutual aid (AA) as an example of how this is done. After all, AA has now been shown to be as effective, if not more effective, than other evidence-based psychosocial interventions. Fittingly for these times, Cutter et al extend the contagion model and highlight the process for a cure:
Here the “vaccine” would not be a pharmacologic injection, but rather a multidisciplinary, cross-sector strategy to combat the spread of opioid overdose and related death similar to public health interventions aimed at combating the spread of an infectious disease.
At the time, the announcement of a vaccine against covid-19 generated phenomenal interest and jubilation. Hope began to be generated. Could we ‘vaccinate’ against drug and alcohol deaths by connecting those who use our services to mutual aid and other community recovery resources? From what we know, this would likely have a very significant impact on outcomes compared to most interventions.
Based on the evidence, connection to mutual aid is already recommended in our drugs strategy, by NICE and in the Orange Book National Clinical Guidelines as well as the ACDM report on Medications in Recovery. But it it happening?
We don’t have to reinvent the wheel here. Public Health England have a great toolkit available to make this easy. I recommend it strongly.

Now, I’m not claiming this approach as an answer to our opiate (and alcohol) deaths. There is no single answer. What I am saying is that we ought to vigorously test out the social contagion/social networking model as part of the range of interventions we are currently adopting – the evidence is already strong and accumulating.
I’d like to see this approach at the heart of all of our interventions and have services held to account on how effectively they link service users into new social networks. I’d like to see some research exploring the impact of adopting a vigorous approach to this. Then I think we would really see change.
Continue the discussion on Twitter: @DocDavidM
This is an updated version of a blog first published in 2020.