
As someone who spent 25 years working for a nonprofit providing long-term residential addiction treatment, I’m of two minds about the state of residential treatment in the US.

On the one hand, our agency struggled mightily to maintain high-quality, ethical, evidence-based care that kept patients engaged and supported them through the treacherous first 1-2 years of recovery. We pioneered services like recovery housing that allowed us to reduce length of stay, get patients participating in community life sooner, reduce costs, and improve outcomes. We did this with unsustainably low reimbursement rates and raised charitable funds to keep the lights on.
On the other hand, I’m very well aware of the shady practices, shoddy practices, and profiteering that occurs in the industry. We put a lot of effort into distinguishing ourselves from those programs and we publicly criticized unethical practices in the industry. I want them to change or get out of the business.
I also know that these kinds of problems are not confined to residential treatment. There are widespread problems in buprenorphine prescribing, recovery homes, lab services, etc.
So… on the one hand, I know there is fraud/waste/abuse and I want it exposed and punished. On the other hand, I know there are good providers out there and I don’t want to throw out the baby with the bathwater. Most importantly, I want people with addiction and their loved ones to be able to navigate systems of care and find treatment of adequate quality, duration, and intensity, and to have their preferences about things like medications respected.
Earlier this year a “secret shopper” study was published and got a lot of attention. It confirmed the unethical practices that I’ve been complaining about for decades, but it bothered me for a couple of reasons. First, it was framed as proof that residential treatment is problematic and should be a thing of the past. Second, it was used to elevate other treatment approaches that also have problems with unethical and shoddy practices.
Rather than just condemning a treatment model (that people seek for rational reasons), wouldn’t it be better to help consumers and referring providers distinguish good providers from bad providers?
Why didn’t they do that? Maybe there weren’t any ways to distinguish?
The Recovery Research Institute just published an analysis of the study and highlight an important pattern:
non-profit admission practices differed considerably from those of for-profit programs. Non-profits were less likely to offer admission over the phone, less likely to exclude patients based on their psychiatric or substance use history, and less likely to use recruitment tactics. Non-profits had longer wait times for admission on average and a lower likelihood of encouraging the patient to take on debt to pay for treatment. In comparison to for-profit programs, non-profit programs have less than half the same-day admission rate and about three times the average wait time. For-profit program costs, on average, were more than twice the amount of non-profit programs per day.
This is all right there in the paper. It’s not even buried in statistical mumbo jumbo. Why didn’t the researchers or the media highlight this to help consumers narrow residential searches and find an ethical provider?
To me, their conclusion indicates a lack of interest in helping patients differentiate between good and bad residential providers.
We found a pattern of high costs and active recruitment, frequently without clinical evaluation, in a national audit of residential treatment programs. Some of these behaviors were more common among for-profit programs, but others were similar across both for-profit and nonprofit organizations. Given that outpatient opioid agonist treatment should often be a first-line treatment for patients with opioid use disorder rather than costly and potentially less effective residential treatment, these findings raise concern about the benefits of investing in access to residential treatment as a policy priority.
Fellow contributor David McCartney’s recent post exposes a flaw in this approach.
His post, reporting on a recent Rec-Path blog post evaluating recovery in policy and practice on both sides of the Atlantic by UK academic, Professor David Best and American economist, Sonia Martin.
They could be understood as suggesting that the we might do well to put less emphasis on the particular modality of treatment and more on its recovery-orientation.
It is notable that almost no funding has been allocated to researching recovery-oriented systems of care in the US or UK in the last decade.
Martin and Best report that the system’s failure to re-orient itself toward recovery has resulted in what some call a “poverty industry.”
The shared concern in both the US and the UK is that increased investment and increased public concern and attention have not led to new ways of thinking but have largely ended up in doing more of the same. More treatment workers, more treatment services and very little of the crucial lessons from recovery – jobs, houses and pathways to community capital and resources. In Scotland, McGarvey (2018)[2] has referred to this as the self-preservation of the ‘poverty industry’.
I’d suggest that good residential providers are recovery-oriented and are effective at addressing things like “jobs, houses and pathways to community capital and resources” in ways that are very rarely seen in other treatment modalities.
We might all be better off if advocates and providers of other modalities paid more attention to the reasons many patients seek residential care and what works well for good residential treatment providers, and then seek to integrate those lessons into their treatment modality. (And, to be sure, we’d all be better of if residential providers, even the good ones, did the same thing.)
It all takes me back 20+ years, with Bill White telling addiction professionals something like, “All these arguments you’re having about TSF vs. CBT vs. MET are stuck in the wrong paradigm. We need to orient ourselves toward recovery.”
It feels like we need to relearn that lesson.
UPDATE: David McCartney commented below. I’m adding it here, to make sure it gets the attention it deserves:
“Given that outpatient opioid agonist treatment should often be a first-line treatment for patients with opioid use disorder rather than costly and potentially less effective residential treatment, these findings raise concern about the benefits of investing in access to residential treatment as a policy priority.”
Mmmm. Does what people want from treatment not matter? Should there not be a menu of treatment options available with risk mitigation for those modalities that are not based on MAT?
Perhaps just as important is the issue around what ‘less effective’ means. In recovery terms, MAT is not strongly evidenced to help people reach recovery goals. While preventing overdose and death is an essential first step, as Eric Strain said: “Not overdosing is an insufficient endpoint for treatment or for societal and medical interventions – it’s a starting point.”
In the UK, as Prof David Best was saying just this week, the policy pendulum has swung from harm reduction to recovery and back again. Unless we do some sensible and joined up thinking, it will continue to vacillate. We need a variety of treatment options because we have a variety of people with different substance use disorders who have varied goals which can vary over time.

Last week, the highlight of my week was not presenting at a conference or completing my part of a hard-worked funding bid, though both of these were satisfying. By far the loveliest thing to happen was a short conversation with an ex-patient who came back to say thank you. She particularly stressed the part that lived experience and having been a peer supporter had played in consolidating her own recovery. I was moved by her gratitude and by what she said.
In Scotland our drug and alcohol policy, Rights, Respect and Recovery, emphasises the important role that lived experience needs to play in helping those with substance use disorders achieve their goals. They and their families are: to be heard (p4), to be involved as key partners (p7), to be realised as key resources (p15), to be seen as experts (p17); to be involved in service design, development and delivery (p31) and must be ‘at the heart’ of a whole family and family-inclusive approach (p41).
Scotland is praised in its approach in a recent blog by UK academic, Professor David Best and American economist, Sonia Martin. Writing at Rec-Path, they evaluate recovery in policy and practice on both sides of the Atlantic. While there are things to celebrate, the ‘disconnect between policy and practice’ concerns them.
Themes I recurrently return to, and which are picked up in their piece, include the tension between public health priorities and what individuals and their families want from treatment, the polarisation of the harm reduction/recovery debate and professional vs. peer roles in supporting recovery pathways.
In their qualitative study[1] of ten peer supporter workers from Ayrshire in the west of Scotland, ‘It’s not 9-5 Recovery’, Martin Anderson and his colleagues found that 8 participants held some negative views around ‘overly medicalised solutions’, whereas belonging to Recovery Ayr played a central role in their recovery, providing meaning and purpose. Peer support allowed integration ‘into a support network not just limited to meetings and appointments’, but peer supporting itself was identified, as it was by my ex-patient, as providing a ‘purposeful social role’ and creating a ‘foundation for recovery’. Small numbers perhaps, but it chimes.
The one thing, arguably not much on the radar, that is highly likely to make a difference to outcomes and reduce harms is this powerful effect of connection to peers, something that should be part of recovery-oriented systems of care. This is not to say that professional interventions are not fundamental to many recovery journeys; it’s just that for many they are a relatively small part of a much bigger picture. I believe that we tend to over-value the role of medical interventions and I say that as a doctor who is passionate about good medical care.
It is notable that almost no funding has been allocated to researching recovery-oriented systems of care in the US or UK in the last decade.
Martin & Best, 2021
We don’t know how good we are at actively connecting our service-users to mutual aid and lived experience recovery organisations (LEROs). We have no monitoring framework in place for this – probably because it’s of little interest or perceived relevance to many in the field. The lack of recovery-oriented research is also something that’s frustrated many of us who’d like to see more of a balance. As Anne Marie Ward, the CEO of FAVOR UK, said at the recent meeting of the All Party Parliamentary Group on recovery ‘we don’t need any more addiction research, we have plenty of that, we need to study what gets us well.’
The group that I chair for the Scottish Government on Residential Rehabilitation recommended that researchers look at this issue recovery outcomes (from residential rehab) specifically. The bottom line is that if the bulk of research in the future continues to be focused on medical interventions then we get the Catch 22 of the oft heard phrase ‘there’s no evidence’ for anything else. Our failure to construct and deliver Recovery Oriented Systems of Care (something that has been called for by one name or another for two decades and something that is much wider than medically-led interventions) is a source of shame for us.
Although there are distinct differences across the pond (notably the way healthcare is paid for through insurance), Best and Martin highlight what they see as the common issues
- The domination of policy and practice by clinical ‘experts’
- The ‘haunting’ issue of harm reduction vs. recovery and the swinging policy pendulum
- Lack of visibility and accountability from policy-setters
- Hegemonic influences of disciplinary backgrounds
- The continuing shadow of the pharmaceutical industry
The emphasis on personal and experiential rather than clinical recovery – and on experiential rather than professional expertise – is where the gulf is most apparent between those with lived experience and medical or policy experts.
Martin & Best, 2021
This is not universal, indeed I am endlessly in awe of colleagues who work in the treatment field whose practice is compassionate, industrious and value-driven, but where they do exist, the attitudes behind this gulf are rarely explicit (though they most certainly can be, with one expert in Scotland describing the potential impact of lived experience in Trumpian style as ‘fake news’). Instead, I hear them in softer ways on a regular basis. I see all such references as subtle stigma.
Martin and Best conclude:
“The shared concern in both the US and the UK is that increased investment and increased public concern and attention have not led to new ways of thinking but have largely ended up in doing more of the same. More treatment workers, more treatment services and very little of the crucial lessons from recovery – jobs, houses and pathways to community capital and resources. In Scotland, McGarvey (2018)[2] has referred to this as the self-preservation of the ‘poverty industry’.”
This is a difficult message to hear. Most of us are doing our best in the face of relentless demand, apparently intractable problems, limited resources and high degrees of risk. The danger is we react defensively. I don’t see these themes as personal attacks or threats to our autonomy, but as calls to to things differently. There must be a middle way here where experts by lived experience and experts by training can all sit round the table as equals. More and more of us now have both qualifications, which can bring its own challenges, but distinct advantages too. With the right approach we can be bridges.
The power of lived experience to introduce hope, establish powerful role-modelling and support others in early recovery is phenomenal. It is patently not ‘fake news’. Think of my grateful patient – she helped herself and others by using her lived experience. She helped our service. She helped me.. The power of lived experience to shape and help deliver policy and services has the same potential, but although you will find it written on page after page of policy and guidance we’ve not yet tested it in a meaningful way.
For professionals and those with lived experience to sit equally around the same table, the table must be big enough, the invitations sent, the door open, the chairs comfortable, and everybody must have a chance to have a say. Crucially, those with lived experience need to be heard in a meaningful way. That is, in a way that can influence policy for the better and help translate it into action.
Continue the discussion on Twitter: @docDavidM
Photo credit: Istockphoto Andrew Johnson. Under license.
[1] Martin Anderson, Alison M. Devlin, Lucy Pickering, Mark McCann & Daniel Wight (2021) ‘It’s not 9 to 5 recovery’: the role of a recovery community in producing social bonds that support recovery, Drugs: Education, Prevention and Policy, DOI: 10.1080/09687637.2021.1933911
[2] McGarvey (2018) The poverty safari: Understanding the Anger of Britain’s underclass. London: Luath Press Limited
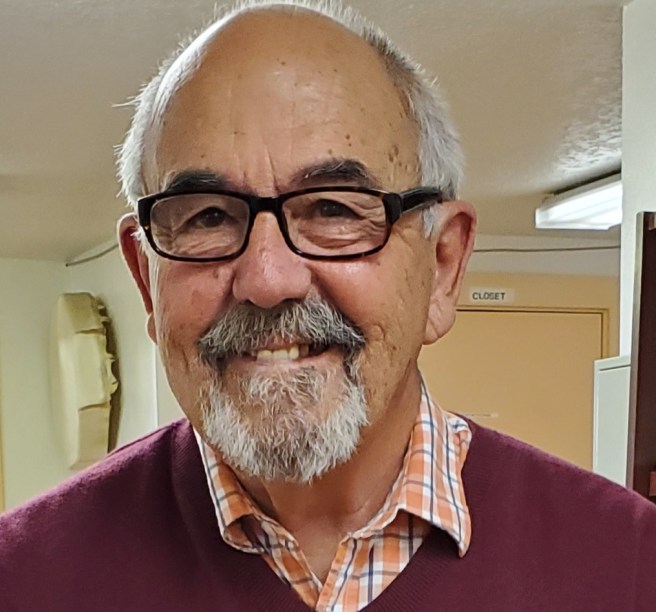
Forward: As I was calling around to set up interviews, Ben Bass came up in several conversations. Several people in attendance told me he was at the historic St Paul 2001 Recovery Summit. When I did this interview and spoke with him about the summit and his recollections of the beginnings of the new recovery advocacy movement, he let me know he was not there. He was involved in planning things at his RCO leading up to the event and implementing them following the summit. The Director of his organization who was not in recovery attended instead. In talking with him, it became clear to me why several people thought he was at the Summit. It was because he was in the initial SAMHSA Recovery Community Support Program grant cohort. While these grants were relatively small, they had a huge impact on recovery efforts in America, Ben was at that time and remains now a leader in these efforts.
Ben is the Executive Director of the Recovery Alliance of El Paso. He began at the Alliance as a volunteer and has served as the director of the Alliance since May 2002. He is the current vice president of the board of the El Paso Coalition for the Homeless; a former member of the board of directors of Faces and Voices of Recovery in Washington, DC; is on the Advisory Board of the South by Southwest Addiction Technology Transfer Center at the University of Texas at Austin. Mr. Bass published in 2009 in Family Community Health Journal an article called Faith Based Programs and Their Influence on Homelessness. In 2011 Mr. Bass was honored at the White House as a Presidential Champion of Change for this work.
This interview helped me to better understand the other major element that helped launch the recovery movement in the United States, the RCSP grants. These SAMHSA grants brought together some amazing people and organizations that have had a huge positive impact on recovery efforts across the nation. The grants were small, but they paid huge dividends in the development of recovery capital across America.
- Who are you and what brought you to St Paul at that time?
My name is Ben Bass, and I am a person in long term recovery, and that means I have not used alcohol or drugs in over 34 years. But it means a whole lot more than that, it means I have been able to hold a job, raise a family and to be a productive member of my community. I was not able to attend the Summit in 2001, there was another person running the Recovery Alliance and she attended instead. I became the director a few months later in 2002. I was very involved with the other RCSP grant holders from across the country, including providing TA on Recovery Community Centers in 2004. I was aware of the influence of the summit on us all and was involved in building on top of the foundation that came out of the summit.
- How did you get involved with the Recovery Alliance of El Paso and the larger recovery movement?
I had been in recovery for a number of years, and it became apparent that we had a lot of holes in the care system in El Paso. I wanted to be involved in addressing those and helping get more people into recovery. So I started to volunteer with others. We were in essence a community action group that developed into a Recovery Community Organization (RCO). I didn’t even know what an RCO was at the time. As it formed, I became a Board member in 1999. It is a long story, but it became apparent in the months after the summit that the director was not a good fit for our RCO. Our board did a search of over 30 candidates and none of them really had the passion for recovery we were looking for. I uttered those three words “I’ll do it,.” I have served in that capacity ever since.
The work we do is so powerful and vital. We are about saving lives. What is more important than that? We have come together to save the lives of our own people – everyone who experiences addiction. That is what gets us out of bed everyday.
The other huge factor beyond the St Paul Summit that drove the movement was the RCSP grant and the amazing people that those grants brought together. Recipients like Don Coyhis of White Bison, Tom Hill of Speak Out: LGBT Voices for Recovery and Phil Valentine of CCAR. I think there were nineteen of us, and we started to talk about stigma and how we were going to address that. We began to develop recovery support services. One of the facets that helped get those grants in place was a Washington Post letter to the editor written by June Gertig about recovery and the need to expand opportunities for recovery in the USA. All the facets came together, the right people at the right time. The rest is history.
There was tremendous energy around what we were working on and that energy propelled our work, both here in Texas and across the country. We would hold a grant meeting and 300 people would show up. When I look back, the people who were running those RCSP projects were key to the development of the recovery movement. They were the right people at the right time, and they worked extremely hard to build something meaningful that is influencing everything we do today in respect to treatment and recovery.
- What did you see as the motivating factors that brought you all together twenty years ago?
As I mentioned, beyond the summit, it was those SAMHA RCSP grants. As far as actual dollars, they were small, but the grants helped bring us all together. Through those grants we developed peer services. As the recovery community came together, we also started to focus on changing negative public opinion about us.
I remember one thing that really galvanized our recovery community here in El Paso and beyond. Christian Dior, the fashion company came out with a fragrance they called “addict.” Their naming of that product and media campaign around it was terrible and really magnified all the horrible negative stereotypes about addiction while also trivializing it. It really upset people. Susan Rook, who was a CNN reporter and the Faces & Voices Communications Director and who was in open recovery contacted us in El Paso and visited. Locally we marched on the local department store and demanded that they pull it from their shelves. They did. We have a lot of military bases in the area, and our advocacy here locally helped to get it pulled from military base here in Texas and at base exchanges worldwide.
Other media sources picked up on it. The executives of Christian Dior ended up having to get on a plane from Paris and fly to DC to meet about it. Dior changed their marketing campaign. Our efforts worked! We saw that we had this immense power to do good things when we all came together. We saw the power of recovery and the possibilities that could come from uniting our community and working towards things that got rid of stigma against us and illuminated the benefits of recovery.
- How have we done in accomplishing those early goals?
We have done so very much to strengthen recovery efforts and save lives; bit we are still just scratching the surface. There is so much work to be done! There is still a whole lot of stigma and discrimination around addiction and recovery. Getting people to stand up and be open about recovery was huge. We have started to put a face on recovery. Getting a CPA or other professionals to talk openly about recovery let the community know that they are in recovery has had a huge positive influence on how we are seen.
I still think that we would greatly benefit from a huge national media campaign on recovery. What happens is it is so hard to keep the gains we have made. Our focus becomes the provision of services and how to fund the work we do, which is always such a challenge. We are very busy people, and a lot of our focus has been on how to keep the things we have already built.
- What do you see our greatest successes to date are?
Patty McCarthy of Faces & Voices of Recovery has done amazing things to help fund our work. Faces & Voices rose out of that 2001 Summit and has helped get people involved across the nation and to some significant political successes to fund efforts nationally. I also see the Association of Recovery Community Organizations as a key organization moving forward. Both of these were born out of our early efforts. I would love to see a summit where we brought everyone together and talk about what our goals and objectives are moving forward. We need to make time we can all sit down together and talk and work creatively to work things out and propel our efforts forward. Something beyond the typical conference with preplanned speakers. An actual sit down to really look at what we have done, what has worked, what has not worked and to plan our next steps. We are all so terribly busy it is a challenge to hold such a space and really use our creativity and knowledge in ways to set the stage for what comes next. I think it is really important that we try and do something like this as a way to set an agenda for the next twenty years. We must recruit new leaders to propel the movement forward.
- What did we miss if anything looking back at those goals?
We missed focusing on more direct confrontation on discrimination and stigma against us. We need to be clear about addition. Addictive drug use is very damaging to our health, our families and our communities and the public can see this with its own eyes. We need to be honest about it. Drug use can be devastating, and people can see it all around them. Society has a lot of antipathy about us, and we have to be careful of how we raise issues around stigma reduction and focus on recovery in ways that highlights what happens when we stop using drugs and alcohol and regain our lives.
So far, what we have missed are opportunities to engage the larger society in mass media campaigns that highlight the power of recovery to transform lives. Having media spots run across the country with Robert Downy Jr, Morgan Freeman and Eminem all taking about recovery and how without it they would be dead. We have yet to transform public opinion about us and to highlight how focusing on recovery can change a lot of things. We are assets in our communities, and we need to take the next step and move recovery efforts forward in ways that capture the imagination of America.
- What are you most concerned about in respect to the future?
I am concerned about the sustainability of peer recovery support services. The funding mechanisms limit what we can do and threaten the future of these services. Here in Texas, there are two billing codes, one for individual peer coaching and one for group peer coaching. We are permitted to bill for fifteen-minute increments and the rates are abysmally low. While the ability to bill is welcomed, it does not pay for the work that is actually done to sustain recovery through the recovery community.
We have been working very hard on trying to figure out other funding mechanisms that actually provide the things that are needed and would therefore be sustainable. The way things are now we end up trying to raise dollars to fund the work we are doing. We need to get private insurance to fund things at levels like they do with medical care so that all of the ancillary services and supports are able to be provided. I do see some movement. Some insurance companies are thinking about it. Perhaps this is one of the things we should bring recovery community organizations together on and to share what we have all learned and what we can do to move the world in this direction.
- What would you say to future generations of recovery advocates about what we did and what to be cautious of / your wishes for them moving forward?
It is important for the next generation to know that we do recover. We are part of the most vital, life altering movements in American history. It is a movement to save lives. I would want the future generation of leaders to know that when we come together, we can do anything! All we must do is do it! If we look back at the last twenty years, we can see that. We can see it if we look back further in history. Look at what Harold Hughes brought together in the late 1960’s and early 1970’s. Look back to the 1940’s and the work of Marty Mann and the formation of the National Council on Alcoholism. History shows us what happens when we come together – we change the world! I would want future leaders to study our history and take what we have done to the next level, if they bring us together, it is certain it will work!
Webinar: Fentanyl in Treatment Courts
Friday, July 16 | 2:00 p.m. EDT
NADCP’s National Drug Court Institute Drug Court U is presenting a free webinar event on what treatment courts and others need to know about fentanyl to better serve participants. The live webinar is presented by pharmacology expert Steve Hanson.
America’s opioid crisis continues to take a toll on communities across the country in the form of overdoses and deaths. The Centers for Disease Control attributes these casualties largely to illegally manufactured fentanyl. Armed with the latest information, treatment courts are well positioned to act against the fast-acting and dangerous substance in their communities.
The webinar offers a comprehensive overview of fentanyl, including its:
- Pharmacology
- Variations
- Medical use
- Street availability
- Overdose prevalence
- Treatment implications
About the Presenter
Steve Hanson, M.S. Ed., is the associate commissioner for courts and criminal justice for the New York State Office of Alcoholism and Substance Abuse Services (OASAS). He is responsible for relationships with the various criminal justice entities, including treatment courts, state and local corrections, and probation and parole. Previously he served as the associate commissioner of treatment for OASAS, with responsibilities for the oversight of state-operated treatment programs, adolescent services, criminal justice, and recovery services. Mr. Hanson has been with OASAS since April 2001, when he was appointed as the director of the John L. Norris Addiction Treatment Center in Rochester. In 2007, he was named director of the Bureau of Addiction Treatment Centers, and in 2009 he was named director of treatment services. He has more than 35 years of experience in the field as a treatment provider, educator, and consultant. His ability to train criminal justice practitioners on drug abuse and treatment has been recognized both nationally and internationally. He has been a NADCP faculty member for nearly two decades.
The post Fentanyl in Treatment Courts: Webinar from Steve Hanson appeared first on NADCP.org.
I stumbled on Sober 21 this morning, which describes itself as “a compendium of essays by, and interviews with, sober musicians”.
The editor’s introductory essay describes the project as follows:
It’s a free resource for musicians who want to begin the journey, or are new to the path of getting clean and sober from drugs and alcohol. … Few professions are as incessantly perilous to the potential alcoholic/drug addict as that of being a musician. You are literally paid to be in rooms with alcohol every night you perform, and are plied with drink tickets and booze in the green room. Alcohol and drug abuse is quite often not only normalized, but expected, encouraged, and even celebrated. … While there are shelves of truly wonderful books dedicated to sobriety, a dearth of material exists that specifically addresses the unique challenges musicians face in getting clean. … Sober 21 brings together a group of musicians that varies in age, gender, race, sexual orientation, musical styles, amount of time sober, and years in the music industry. What they have in common is that they were actively addicted to alcohol and drugs, and that they share here that they are now free from that addiction.
I found the essay by Peter Hook (Joy Division / New Order) interesting and really enjoyed the interview with Darryl “D.M.C” McDaniels (Run-DMC).
I’m looking forward to reading the rest. Enjoy!

My Test, My Way – My contribution to Ending the HIV Epidemic in the U.S.
Kristin Roha, MS, MPH, SAMHSA Public Health Advisor for HIV
On June 27th of each year, National HIV Testing Day (NHTD) reminds us of the importance of HIV testing and gives us the opportunity to share HIV testing resources. Getting tested for HIV is easy, fast, confidential, and safe, and is the first step in knowing your HIV status. For people who test positive for HIV, getting tested is the gateway to accessing lifesaving treatment. For people who test negative for HIV, getting tested can provide empowering information that can help make them decisions about sex, drug use, and health care. For people at risk for HIV, a negative test can also be the gateway to accessing powerful preventive tools, including pre-exposure prophylaxis (PrEP).
SAMHSA’s mission is to reduce the impact of substance abuse and mental illness on America’s communities. People with mental illness and/or substance use disorder are at increased risk of getting HIV, and of passing the virus on to others. From SAMHSA’s National Survey on Drug Use and Health (NSDUH), we know that the prevalence of mental illness is higher among people living with HIV than among the general population; mental illness is also is linked to behaviors that increase the likelihood of getting HIV. We also know that the prevalence of substance use is higher among people living with HIV than among the general population, and that substance use disorder – especially injection drug use – can increase the risk of getting HIV. For this reason, SAMHSA is a proud partner in the Ending the HIV Epidemic in the U.S. initiative, which aims to reduce new HIV infections in the U.S. by 90% by 2030.
Substance use disorder and mental healthcare practitioners like SAMHSA’s grant recipients and partner organizations serve on the front lines of the HIV epidemic and can play a vital role in ensuring people at risk for HIV receive an HIV test. SAMHSA has long encouraged substance use disorder and mental health treatment providers to integrate HIV testing into their routine standard of care, and we have made it a requirement for some of our grants. The CDC recommends that that people who inject drugs (PWID) and share needles, syringes, or other drug injection equipment should get tested for HIV every year, but in 2018 only 55% of PWID had been tested for HIV in the past twelve months. This year on NHTD, SAMHSA again encourages all substance use disorder and mental health treatment providers to test new clients for HIV and hepatitis at intake.
The theme for this year’s NHTD is “My Test, My Way,” because today there are more HIV testing options available than ever before. This year the COVID-19 pandemic changed the way people access healthcare, including HIV testing. Though many of SAMHSA’s grant recipients were able to remain open and offer in-person testing, others experimented with offering HIV self-tests via contactless pickup or through the mail. Now, though many facilities are open and able to offer HIV testing in person again, it’s important to seek testing in whatever way makes you feel the most comfortable. If you would like to receive an HIV test in person, you can find a testing provider through the CDC’s Get Tested website. Get Tested also has resources to help you find condoms and PrEP providers in your area. If you would prefer to get tested at home or at another preferred location, HIV self-tests can be used wherever you choose. Right now, many local health departments and community-based organizations, as well as the CDC, are distributing free HIV self-testing kits through a program funded in part by the Minority HIV/AIDS Fund. Finally, if you, or someone you know, is seeking help for substance use or mental illness, SAMHSA’s Behavioral Health Treatment Services Locator can help you connect with treatment programs in your area.
Testing, including self-testing, is one of the many tools we have at our disposal for ending the HIV epidemic. We are closer to reaching this goal than we have ever been. SAMHSA would like to take this opportunity to thank our grant recipients and partner organizations for your perseverance and flexibility in ensuring that your clients were able to get tested for HIV over the past year. We would also like to encourage everyone at risk for HIV to take the opportunity provided by NHTD to get tested in a way that works best for you – whether it’s self-testing in your own space of finding a testing site nearby. Together we can contribute to ending the HIV epidemic, one HIV test at a time.
From the recently updated NIAAA fact sheet on alcohol and health:
An estimated 95,000 people (approximately 68,000 men and 27,000 women) die from alcohol-related causes annually, making alcohol the third-leading preventable cause of death in the United States. The first is tobacco, and the second is poor diet and physical inactivity.
Of course, there are lots of other social costs associated also with alcohol and tobacco.
This should prompt reflection and planning as move toward decriminalizing and celebrating other drugs.

We are pleased to announce the release of our newest Tips & Tools for Recovery that Works! video the Keys to Happiness Part 2.
Health and happiness are desired outcomes of successful recovery, and SMART Recovery has compiled a list of 12 tips for greater happiness that can help anyone. In this Part 2 of the series, we discuss the last 6 tips.
Watch the Keys to Happiness Part 1 video.
Watch the Unconditional Other Acceptance video.
Watch the Unconditional Life Acceptance video.
Subscribe to the SMART Recovery YouTube Channel
Video storytelling is a powerful tool in recovery, and we are proud to share our SMART Recovery content free-of-charge, available anywhere, on any device. Our videos hope to inform, entertain, and inspire anyone in the recovery community.
Subscribe to our YouTube channel and be notified every time we release a new video.
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments
we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!

Recovery: a lived experience of improved life quality and a sense of empowerment
Best & Laudet
When it comes to drinking problems, men and women have differences. Women tend to binge, have higher pre-existing trauma levels and can suffer more (or different) kinds of stigma and discrimination. They are also more vulnerable to physical complications and have greater mental health co-morbidity. Alcohol-related mortality is higher. In my work I’m seeing more young women with alcoholic cirrhosis of the liver than ever before – a worrying trend.
Gender norms and societal expectations often result in stigmatisation when the ‘alcoholic woman’ deviates or is unable to fulfil prescribed gender roles (i.e. wife, mother). Such stigmatisation results in a reluctance to ask for help.
Women and recovery
Recovery can also be different. Women face barriers to treatment. Issues around childcare and fear of losing custody, domestic violence, trauma and unemployment can act as deterrents. In addition, it has been found that some services are more tailored to men than women. Recovery capital resources may be less available to women who can experience ‘oppressive experiences of social control’.
Wanting to know more
It’s really good to see alcohol research focussing on women. Zetta Kougiali, Alicia Pytlic and Kirstie Soar took a look[1] at qualitative studies which examined women’s pathways into dependence and then into recovery. They quote the Best and Laudet[2]description of recovery as ‘a lived experience of improved life quality and a sense of empowerment’.
The authors wanted their study to offer valuable knowledge towards understanding the different needs, mechanisms, and factors that can facilitate or hinder women’s recovery.
The research
They examined 23 published studies, including one from Scotland. They identified 4 themes.
- The pre-drinking ‘self’
Kougiali and colleagues found that women linked trauma and victimisation experiences (e.g., childhood sexual abuse, growing up in abusive families, emotionally absent parents) in earlier life to the development of their drinking problems. These experiences had generated intense shame and feelings of not belonging, inadequacy and inferiority.
The experience of having to conform to gender norms, feeling choices were limited and lack of ability to allow the ‘real self’ to emerge were all cited as relevant.
2. Alcohol as a corrective agent
Drinking was used as a technique to ‘correct’ negative feelings through the creation of a ‘substitute self’, a ‘substitute reality’ and temporary empowerment.
3. Escalation of drinking and the dependent self
Although alcohol was initially used to ease the difficulties, a tipping point came when this could not be maintained. Paradoxically, the use of alcohol started to create the same problems that it had been used to tackle, resulting in despair and hopelessness linked to shame and stigma. A sense of being trapped developed.
4. The recovering self
The process of recovery happened when power was transferred from external things, like alcohol and other people, back to ‘the self’. Although turning points varied, they were connected in the sense that a belief that drinking was no longer sustainable developed. The authors say, ‘Participation in recovery groups helped gradually move from concealing perceived problematic aspects of personality to increased self-expression, sense of belonging, and empowerment.’
Going to recovery meetings also helped develop a social network that countered the loneliness and emptiness that can accompany early recovery.
Women’s accounts revealed their understanding of recovery groups as spaces of collective as well as individual empowerment.
Kougiali et al, 2021
According to Krenzman et al[3], women make up a third of Alcoholics Anonymous membership and do better than men in terms of outcomes. However, for women attending AA meetings there can be controversy over the concept of powerlessness. In this study, participants identified powerlessness as a helpful concept, as they did other features of the AA programme, such as self-awareness and self-reflection, group membership (sense of community and belonging) and sponsorship (sense of connection).
There were benefits to attending women-only meetings, though interestingly, most women stressed the importance of attending mixed meetings too, even though some women experienced distress when disclosing their past in mixed meetings. This led the authors to suggest that women with adverse experiences and those in early recovery should be ‘informed both of the implications and potential benefits of participating in mixed-gender meetings’.
Summary
“Alcohol was initially used as a corrective agent and as a tool of temporary empowerment, regulating structural and familial imbalances. However, drinking became progressively compulsive and overpowered every aspect of life. Initiation of recovery was often hindered by shame and stigma and facilitated by belonging to and being accepted by recovery groups and a revision of ‘the self’ within wider social structures.”
Continue the discussion on Twitter: @docDavidM
Photo credit: fizkes/istockphoto. Under license
[1]Zetta G. Kougiali, Alicja Pytlik & Kirstie Soar (2021) Mechanisms and processes involved in women’s pathways into alcohol dependence andtowards recovery: a qualitative meta-synthesis. Special issue on mechanisms and mediators of addiction recovery, Drugs: Education, Prevention and Policy, DOI: 10.1080/09687637.2021.1904836
[2] Best, D., & Laudet, A. (2010). The Potential of Recovery Capital. Royal Society of Arts.
[3] Krentzman AR, Brower KJ, Cranford JA, Bradley JC, Robinson EA. Gender and extroversion as moderators of the association between Alcoholics Anonymous and sobriety. J Stud Alcohol Drugs. 2012 Jan;73(1):44-52.
Check Out the Latest RISE21 Program and More
As the country reopens and travel restrictions ease, we’re moving full-steam ahead with RISE21! The preeminent conference on addiction, mental health, and justice reform, RISE21 will be held August 15-18 at the Gaylord National Resort & Convention Center in National Harbor, Maryland.
Register and secure your housing today!
RISE21 Program
The RISE21 program has been updated to reflect the latest and greatest on a wide variety of session topics and learning tracks. Attendees can earn up to 24.5 hours of continuing education! RISE21 will feature content such as:
- Equity and inclusion
- Alternatives to jail sanctions
- Legalized marijuana and treatment courts
- Law enforcement–specific sessions
- Veteran-focused sessions
- …and much, much more!
The post RISE21 Program Now Available appeared first on NADCP.org.