
April Showers Bring May Flowers, How to Get Through your “Lows” (Depression/Anxiety)

When you were in active use, you probably used substances to numb your emotions. In recovery, you must learn how to master coping with these emotions instead of letting them be the master of you. Feelings are a difficult thing for all individuals to manage, but it is known that they are especially difficult for those in recovery.
Substances alter the chemicals in your brain, long after the periods of active use. Establishing an emotional baseline and managing the highs and the lows will be challenging, but not impossible.
Here are FIVE ways to manage your “low” moments while in recovery:
Pick up the Phone and Call…Before You Want To
Most of the time, you probably don’t want to “bother” others with your seemingly small problems. You might be annoyed with your family, angry with a situation at work, or suffering from lower-than-usual self-esteem. It’s easy to convince yourself that situations like these are minor inconveniences that aren’t worth calling your sponsor or friends in recovery about.
What you might not realize is, these situations, if left unaddressed, can build in your mind. As you work to suppress them, the negative emotions surrounding them can compound and become something much bigger than they ever needed to be—bringing you to a low point. Avoid this by being open with others. Call those in your support network when things are good, when things are bad, and when things are boring. You may find that as you begin talking, subconscious feelings come to the surface. Something you say might even help someone else without you realizing it. Call a friend today, before you’re in the low point.
Practice Self-Care
When you’re feeling low, basic tasks can become mountains to move in your mind. Getting out of bed and eating can be difficult in those depressing moments. Even if it is the very last thing you want to do, most of the time spending a small bit of time on personal hygiene (showering, a hot bath, brushing your teeth, a face mask, etc.), preparing a hot meal, and getting your body moving can be the very thing you needed to reset and to get to feeling a bit better.
Small actions of care for the self lead to big emotional changes. Practice repeated routines and actions each day to care for yourself. This might be a 30-minute walk, trying a new recipe, or sitting down with a cup of hot herbal tea in the evening. Do something for you, daily, to increase your feelings of confidence and self-worth.
Stay Spiritually Fit
Your mind can become clouded, especially when you’re feeling down. It can be difficult to think logically or to even think at all in those moments. Don’t forget to turn your problems, no matter how “small” over to your higher power as you understand it.
Meditation, prayer, mindfulness, yoga, and spending time in the sunlight can all be great ways to ground yourself and to combat the feelings of anxiety and depression that take over during “lows.”
Go to a Meeting
This may seem obvious, but don’t talk yourself out of a meeting. Usually, when you want to go the least is when you need to attend one the most. Feeling “low” isn’t just an emotional feeling, it can be physical and all-encompassing lethargy and lack of energy or motivation to do anything. You will always feel better after a meeting, so reach out to a friend in your network and let them know what you’re going through. If you need extra support, ask them to attend with you.
Seek Professional Help
Some “lows” cannot be managed alone. Be sure to be open with your small group, psychiatrist, doctor, and counselors about what you are experiencing. Professionals are trained to handle the emotional distress that you are facing far better than yourself or anyone else. There’s no way to know exactly what is causing your distress without talking with a professional, it may be related to your diet, sleeping habits, or other medical issues. Remember, being honest with those around you is always the best way to begin feeling better.
***
For more information, resources, and encouragement, “like” the Fellowship Hall Facebook page and follow us on Instagram at @FellowshipHallNC.
About Fellowship Hall
Fellowship Hall is a 99-bed, private, not-for-profit alcohol and drug treatment center located on 120 tranquil acres in Greensboro, N.C. We provide treatment and evidence-based programs built upon the Twelve-Step model of recovery. We have been accredited by The Joint Commission since 1974 as a specialty hospital and are a member of the National Association of Addiction Treatment Providers. We are committed to providing exceptional, compassionate care to every individual we serve.

My organization, PRO-A recently joined 36 other state and regional recovery community organizations across America and sent this letter to Congress to educate them on the woefully inadequate funding for grassroots recovery community organizations. Disparate funding is the norm even as Billions of supplemental dollars flow out to the states. Even when these allocations specifically mention recovery community organizations, they consistently fail to get resources to recovery community organizations at any equitable level. The funds generally end up elsewhere. This must change.
Here in Pennsylvania, not one single dollar from the federal (SAPG) block grant is allocated for our statewide recovery community organization. Not even one penny. Other statewide recovery community organizations are experiencing similar dynamics. As the letter to Congress from our 37 recovery organizations states:
“Block grants require states to have consumer advisory committees, yet without supported
statewide recovery community networks ensuring leadership, advisory structures become
rife with tokenism. Funding, intended to support our efforts when passed through the SSA
system more often than not go to large foundations, long-standing clinically focused
providers, and academic institutions well connected and well poised to secure these funds
yet with little or no insight into local recovery needs of communities.”
We are experiencing systematic disenfranchisement. Millions of dollars goes to large foundations and politically connected groups, while recovery community organizations buy ink for their deskjet printers with social media funded campaigns. Recent grant applications for recovery support services in our state include treatment programs as eligible and have short turn around periods, which disadvantages small grassroot recovery community organizations and advantage large treatment organizations who can write grants quickly. These are dynamics that are unfortunately widespread across the United States. We should have broad conversations about what gets funded, and what equitable means in respect to funding allocations that support grassroot recovery community organizations in meaningful ways.
The new recovery advocacy movement was founded by the recovery community and oriented towards inclusion of recovery communities, in all our diversity in all elements of care planning, provision and evaluation. Improving care and recovery rates cannot occur unless there is meaningful inclusion of our community in matters that impact us. As I wrote about last year with recovery historian Bill White in this piece on Recovery Representation:
“Supporting and strengthening long-term recovery across multiple pathways of recovery and diverse cultural contexts must remain a central focus of our efforts. This is “the commons” of our movement for which we need deep, equitable, and inclusive representation in matters that effect our lives. Nihil de nobis, sine nobis is Latin for NOTHING ABOUT US WITHOUT US and has been a rallying cry for democracy and disenfranchised groups for over 500 years. It means that no policy should be decided without the full and direct participation of those affected by that policy. We must ensure that our voices are included in all systems addressing alcohol- and other drug-related problems.”
Recovery community organizations at the state and local levels are vital to the kinds of systems changes we need. We expand recovery capital, not just on the individual level where most of our care systems are beginning to understand the role and function of recovery management, but on the systems level in the community level as well. These functions are critically needed and a foundational element of statewide recovery community organizations, yet they are not being systemically funded at a time when such infrastructure development has never been more vital. This must change.
We are not experiencing anything close to the level of inclusion we need to move our systems beyond the kinds of exclusionary policies and barriers that have plagued it over the last 50 years. No system can change without meaningful inclusion of the impacted community, including persons in recovery and recovery community organizations. Exclusion equals discrimination, there is no way to sugar coat that. The recovery movement came from the recovery community and occurred because are systems were not meeting the needs of persons with addictions. We have not made enough progress on those goals. We need to keep our eye on the prize and insist that recovery community organizations at the state and local levels are funded in stable and equitable ways that allow them to do this vital work.
Nihil de nobis, sine nobis – Latin for NOTHING ABOUT US WITHOUT meaning that no policy should be decided without the full and equitable participation of those affected by that policy. We must ensure that our voices are included in all systems addressing alcohol- and other drug-related problems. Anything less is unacceptable.

Getting connected to others is good for us. Finding new social networks is an important part of many recovery journeys. Mutual aid recovery organisations are key to this process. In the UK, referring to mutual aid is embodied in our National Clinical Guidelines, National Drugs Policies and is endorsed by the National Institute for Health and Care Excellence (NICE). There are evidenced ways to get people there more effectively. A few years back researchers took a look[1] at how young people respond to 12-step participation, reasons for not going and reasons for discontinuation.
Advantages
The authors start out by laying out the evidence for beneficial outcomes of participating in 12-step mutual aid:
Studies in the addiction treatment field have shown that participation in 12-step mutual-help organizations (MHOs) following treatment, such as Alcoholics Anonymous (AA) and Narcotics Anonymous (NA), is related to higher rates of remission from substance use disorder (SUD) and simultaneous reduction in health care costs.
They point out that while several studies support the benefits of 12-step participation, they don’t provide much in the way of guidance in how to get people there and keep them engaged more effectively.
Questions
The authors set out four questions to be answered through the study:
- What do young adults find most helpful about attending 12-step MHOs?
- What do young adults like least about attending 12-step meetings?
- What reasons do young adults report for discontinuing 12-step group attendance?
- If a young adult never attended a 12-step meeting, what are some of the reasons for not attending?
The study recruited 302 young adults (18-24 years) going into a residential treatment programme in the USA. Almost three quarters were male. Patients were interviewed on admission, on discharge and at 3, 6 and 9 months post discharge with good follow-up rates.
Drugs used
The most commonly reported “drug of choice” was alcohol (28.1%) and marijuana (28.1%), followed by heroin or other opiates (22.2%), cocaine or crack (12.3%), and amphetamines (6.0%). Small proportions reported benzodiazepines (2.0%), hallucinogens (1.0%), or ecstasy (1.0%) as their drug of choice.
Findings
Around a third of the young people had been to a 12-step meeting on entry to treatment. What about on follow-up?
At the 3-month follow-up assessment, 87.6% of the sample (n=212) attended at least one 12-step meeting in the past three months, 81.0% of the sample (n=175) attended at least one meeting in the three months prior to the 6-month follow-up assessment, and 75.5% of the sample (n=162) attended at least one meeting in the three months prior to the 12-month follow-up assessment.
What was most helpful?
- Removing a sense of isolation
- Validating experiences
- A sense of belonging, acceptance and validation
- Installation of hope (being inspired/encouraged by another member who has a similar problem).
- Altruism (members help and support each other).
12-step specific responses were rare leading the authors to conclude that ‘general group therapy factors were more important to these young adults in early recovery/post-treatment.’
What did they like least?
- Meeting structure (length, repetition)
- Having to motivate oneself to get there
Interestingly, less than 1% of young people found meetings unhelpful.
Why did they stop going?
- Logistical barriers (e.g. lack of transport)
- Low recovery motivation and interest
Why did some never attend?
- Didn’t need treatment
- Don’t have a problem
Key quotes from the paper
“These findings are in line with research that has found that the social aspect of MHOs is associated with long-term abstinence by increasing positive types of support and promoting engagement in larger recovery networks”
“Clinicians can highlight that 12-step specific content was rarely cited as a reason for discontinuing 12-step attendance among young adults”
“Findings may inform and enhance strategies intended to engage young people with community-based recovery focused 12-step MHOs and ultimately improve recovery outcomes”
Reflections
If the study were repeated in the UK, then I think we would see that fewer young people had ever been to a mutual aid meeting. We know that there is often a broken bridge between treatment and recovery communities. Then there is the fact that differences in culture mean that we can’t simply translate this research from across the Atlantic.
It’s encouraging that the vast majority of young people found 12-step meetings to be of help in recovery. Some of the obstacles the research uncovered can be tackled as the paper suggests.
Prejudices against 12-step mutual aid continue in the UK even in the face of the strength of the evidence and professional attitudes can and do act as a barrier to access. Despite cultural discrepancy, this study should encourage us to try harder to get young clients in treatment engaged with 12-step and other forms of mutual aid like SMART and LifeRing.
Note: this is an updated version of an earlier blog post.
Continue the discussion on Twitter: @DocDavidM
[1] Labbe AK, Slaymaker V, Kelly JF. Toward enhancing 12-step facilitation among young people: a systematic qualitative investigation of young adults’ 12-step experiences. Subst Abus. 2014;35(4):399-407. doi: 10.1080/08897077.2014.950001. PMID: 25102256; PMCID: PMC4268407.
Bill Greer came up through the ranks of SMART Recovery. He started as a participant in 2012, then became a facilitator, then Regional Coordinator, and joined the Board of Directors in 2017. He is currently the President of the Board. As SMART releases its 2021-2022 Strategic Plan to the community, he knows the importance of implementing goals that will shape SMART’s future.
In this podcast, Bill talks about:
- The 2021-2022 Strategic Plan
- Coming up through the ranks of SMART
- The lived experience of SMART
- What the Strategic Plan means
- How the Strategic Plan achieves the SMART mission
- How the Strategic Plan is aimed towards supporting our volunteers
- A decade of incredible growth and why the Strategic Plan is necessary for continued growth
- Addressing uncomfortable and challenging questions
- Why it’s critical to shift to a fund development culture
- Making SMART a household name
- His meaning of Life Beyond Addiction
- What the Strategic Plan means to you and how to take action
Additional resources:
Click here to find all of SMART Recovery’s podcasts
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @ 800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!

Holly Paulsen’s experience in the U.S. military was fulfilling but stressful. A common phrase in the military is “Drink About it, Don’t Think About it.” This led to personal consequences and eventually led her on a path to recovery that included SMART Recovery and living a Life Beyond Addiction.
Subscribe to the SMART Recovery YouTube Channel
Video storytelling is a powerful tool in recovery, and we are proud to share our SMART Recovery content free-of-charge, available anywhere, on any device. Our videos hope to inform, entertain, and inspire anyone in the recovery community.
Subscribe to our YouTube channel and be notified every time we release a new video.
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @ 800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!

Lise Roemmele had a choice to make. Desperate to help a loved one in active addiction, she could allow them “hit rock bottom” or look for a way to help her loved one and herself.
SMART Recovery’s Family & Friends program offered exactly what Lise was looking for. After attending meetings as a participant and seeing the incredible progress in her loved one’s recovery and her own ability to help him, Lise decided it was time to give back. She took the SMART Recovery Training Family & Friends Training and now leads amazing meetings on her own.
Learn more about becoming a SMART volunteer.
Learn more about the Family & Friends program.
Subscribe to the SMART Recovery YouTube Channel
Video storytelling is a powerful tool in recovery, and we are proud to share our SMART Recovery content free-of-charge, available anywhere, on any device. Our videos hope to inform, entertain, and inspire anyone in the recovery community.
Subscribe to our YouTube channel and be notified every time we release a new video.
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!
Have an Exemplary Treatment Court Program? Become a Mentor Court!
Applications due May 14, 2021
NADCP is seeking exemplary treatment court programs to join our national network of mentor courts. If you think your program exhibits the best qualities of the treatment court model, apply now to be a mentor court!
Visit the application page to learn more about the requirements and benefits of becoming a mentor court. Before applying, watch an informational webinar recording with National Drug Court Institute Director Vanessa Price and current mentor courts.
About NADCP Mentor Courts
NADCP mentor courts are exemplary adult drug courts, tribal healing to wellness courts, co-occurring disorder courts, and veterans treatment courts that serve as national models for three-year terms. These top-tier programs play a significant role in NADCP’s training, technical assistance, and research efforts.
As a mentor court, your program will:
- Host team members from other jurisdictions for both in-person and web-based visits
- Participate in research and media opportunities
- Serve as a national model
- Provide peer-to-peer learning opportunities
- Receive fee wavers and travel costs for two program representatives to attend RISE for each of the three years
The NDCI Mentor Court Program is supported by the Bureau of Justice Assistance, Office of Justice Programs, U.S. Department of Justice.
The post Become a mentor court! appeared first on NADCP.org.
My human geography classes have me thinking a lot about the connections between people, place, and the affective dimension or field that arises from communities with a shared purpose, location, and hope. When combined with ideas about develecology1 and the ways identity is shaped and formed through and across dimensions of various social roles, I have come to understand my own recovery experiences in a new light in recent years. I wish to share the insights I have found.

The town where I achieved lasting recovery is an exceptional place. Kerrville, Texas, is a city of about 50,000 people, straddling the banks of the Guadalupe River in the rolling scenery of the Texas Hill Country. If you’ve never been to the Texas Hill Country, words really would never do it justice. It is situated between the European frontier settlement of Fredericksburg, which has preserved its German roots almost intact, Centerpoint, an old farming community, and Ingram, which serves as a gateway to the Edwards Plateau and ensuing canyons and mountain to the southwest.
To the east of Kerrville lies farm and ranch land extending to San Antonio’s outskirts along IH-10. The land smooths out eastward. To the west and southwest, limestone hills, valleys of amber wild grass, cedar, rock, and clear water streams. The terrain is dotted with enormous ranches, hunting leases, and exotic game farms. You are just as likely to see a Zebra or a Giraffe as you are to encounter a rattlesnake or wild hog. To the south begins the gradual declination toward the Mexican Frontier and the Chihuahuan desert. North will take you into the outskirts of the Capitol city.
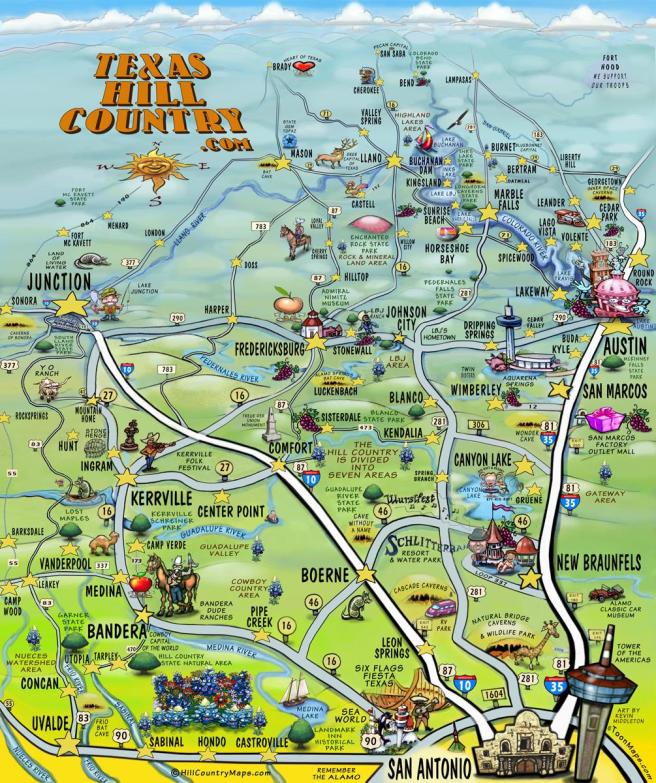
In many ways, Kerrville is a hub from which one can strike out in different directions and experience a complete variety of terrain. Kerrville is a gateway to the vast array of landscapes that Texas has to offer. Metaphorically, Kerrville serves as another gateway, one where a person may pass from the dark lands of addiction into the sunlight of recovery.
It isn’t just the terrain that makes Kerrville a special place. There are five treatment centers nestled in the hills and valleys surrounding the town. The town itself is a retirement community, and as such, requires youthful workers to support the retirees. Kerrville has no less than 25 privately owned sober houses operating at any given time. There is an accountability system between the treatment centers and the halfway houses in town. Since such homes depend on referrals from local treatment centers, their reputation has to be top-notch. It is not uncommon to welcome a treatment center to come by and talk with the residents. Being delisted from local treatment because your sober living house has a poor reputation is effectively a death knell for your operation. Members of the recovery community generally own these sober homes, and as such, they are governed by the principles of the recovery community. The houses are expected to be fair, accountable, and well managed.
Ethically speaking, one’s sober home operation is an extension of one’s embodiment of recovery values. The recovery community police shady business, greed, and unethical behaviors. The quickest way to get run out of town is to screw over vulnerable people. Still, one’s reputation in business or recovery is never entirely written off. Doing an about-face, cleaning up one’s operation, and making amends to the community can put a person back in the graces of the townsfolk and the treatment centers. There are limits, of course, truly bad operators, and fly-by-nighters are banished. Many predatory outfits have tried to set up an operation there only to be completely shut out. Sober house owners are a tight community of owners who collaborate rather than compete. One does not open a sober home in Kerrville with profit in mind. Most of the recovery homes run on the thinnest of margins. They are always teetering on the edge.
The idea is simple: offer a bed to people who have no place to go or for whom to return to their hometown would be a bad idea. Beds go for a few hundred dollars a month. One must work, attend recovery support groups, pay their rent, help out around the house, and be accountable to housemates and the recovery community. The low rent means that one can afford their bed based on even low-wage jobs in town. There are several businesses in town as well that cater to hiring people in recovery.

The usual arrangement is that one goes from a local treatment center into a sober house in town, gets a job, goes to meetings, stays for about a year, and then moves on. It is a staging area for full integration back into the world. It is impossible to go anywhere in town and not encounter other people you know from the recovery community. In this way, the town itself, the economy, the living space are a microcosm or an extension of the post-treatment support space. You might work on a construction crew with people you went to treatment with or encounter a friend of Bill’s behind the register at the local convenience store. In general, the people and business owners in recovery provide opportunities to get back on their feet.
The often-invisible and informal network of the recovery community may help find you a job, a place to live, or help you buy a cheap car to get to work. A principled symbiosis exists between the recovery community, local treatment centers, local business owners, and the larger city. Relapsing in town is public and embarrassing, but many a 12-Step call has been made to the local motel, where the person is given a host of options for getting back into treatment, back into a sober house, aftercare, or all three. In many ways, if you are going to relapse post-treatment, you are fortunate to do so in such an understanding place. They care, and they will do whatever they can to get you the help you need.
From Kerrville, many head to larger cities after getting their lives together. They might land a job in San Antonio or Austin, or they might return to school through collegiate recovery programs (CRPs) found at every state institution throughout Texas. The state university system has adopted a mandate for recovery communities on campus. People in recovery can find scholarships through CRPs simply for being in recovery. From 30-60 days in treatment to a year in sober living in Kerrville and then onto a CRP could keep one in the recovery pipeline for five years or more while sequentially addressing clinical needs, community reintegration, and increasing recovery capital. It is no wonder that so many successful recovery trajectories come out of this pipeline, and it is in many ways an ideal model for abstinence-based recovery.

The entire pipeline consists of a mix between public and private, for-profit and non-profit, formal and informal systems; all centered on the fundamental and altruistic belief that people in recovery deserve every opportunity to rebuild their lives, and succeed, so long as they are willing to work toward a goal of long term recovery. I am sure other such arrangements exist in other places, though I cannot think of one. As a scientist and as a beneficiary of this specific pipeline, I have come to appreciate how truly fortunate I was to be plugged into this pipeline. I read accounts of shady brokers, exploitative treatment centers, places like Florida, and elsewhere. I find myself genuinely grateful that there are places, spaces, communities, and people that provide a counternarrative to such shameful practices. And while Kerrville and the recovery pipeline that runs through the Texas Hill Country isn’t perfect, it is by far one of the greatest assemblages of recovery-centric communities and institutions in existence.
I imagine a day where such a pipeline is a tangible offering to anyone seeking long-term abstinence-based freedom from the struggle and misery of addiction. I think many more people would be attracted to recovery if they were offered such a pipeline. Imagine being able to tell people on day one that they’d not only still be in recovery within five years but also that they would be given opportunities to achieve all the dreams they had been denied in their active addiction. After all, what we wanted was a better life. The systems and supports we offer people seeking recovery must be able to offer the means to a better way of living and growing. Sometimes, it is just that simple.
1.) Shelton, L. (2018). The Bronfenbrenner primer: A guide to develecology. Routledge.
During their ugliest, most severe, and worst stage of their addiction, the start of their recovery is invisible to everyone else. The nascent recovery within them (perhaps nothing more than a simple moment of clarity) seems to have its own voice and is already speaking to them. Later, that suffering person speaks to others about their recovery. But those others say to themselves and to each other, “They’re not in recovery. Not yet. And they sure aren’t in recovery just because they say they are.” In this way, being discounted improperly, they are a Recovery Orphan.
What might some consequences be? Perhaps the one still suffering who has recovery inside picks up a hint of that denigration (almost like they can smell the judgment in the spaces between the words they hear). And then that person retreats to stay in the shadows. And perhaps they are lost to an early death. Or simply lose years of their life existing inside a tornado of a continued pattern of reckless use.
At their most mature-looking and best height of their false, inauthentic, and carefully manufactured persona (that is a mere replica of full recovery and might be taking place during years or decades of continuous abstinence) their addiction is invisible to everyone else. They are not sharing vulnerably. They are not giving or receiving from their place of need and vulnerability. But others might say to themselves and to each other, “They’re in really good, mature, full recovery.” In this way, being affirmed improperly, they are a Recovery Orphan.

What might some consequences be? Perhaps years into this dynamic they violate their abstinence with 4 fingers of fine scotch and then end their own life with a firearm. Or perhaps they merely lose years of their life by living inside a hall of mirrors, and keeping up appearances. But all the while, by all appearances, they are seemingly in the best functioning of their life, connected and re-connected, while focusing on service and giving back.
Recovery Orphans
In the Stages of Change model, the first stage is called “pre-contemplation.” This is the phase of active addiction illness when the person is seemingly immune to the facts of reality and apparently are not motivated for positive change by experiencing any additional pain or negative consequences of continuing to use. They aren’t even on the fence. They aren’t even contemplating change.
But what comes before pre-contemplation? To me, the answer is “Closure”. And the kind of process that would produce the level of closure we find in active, full addiction illness tells us something. It tells us that there was a person inside who lived through the experience of their own slow process of closure. To me, that person is still inside there. And further, that process of closure might even plant or hold seeds of recovery. How so? The memories or voice of a real-self, or the ecology that was lived in before the process of closure gained momentum, and the lived experience of the process of their own slow closure, might be a form of recovery capital. That is to say, those memories might be a point of contrast still inside the person, even at their eventual worst.
Have we ever met someone in the years during which they were experiencing slow and progressive closure? Should addiction professionals advise such a person that they should do more research and continue to use? Does that person deserve their seeming self-imposed fate as a recovery orphan?
And what about closure that takes place later on?
In the Stages of Change model, the last stage is “maintenance”. This is the phase of addiction recovery where sustaining the positive determination and action that produced recovery and initially sustained it becomes internalized and takes less effort to keep.
But what comes after maintenance? Can recovery become false? Can closure creep in? Can someone that far along begin to develop a type of unhealthy closure? And if so, should such a person be turned over to their self-assigned fate as a recovery orphan?
Recovery Orphans
Notes in reaction to “What Is Metaphysics”?
- Each thing contains everything.
Taken as a whole, our field contains at least both addiction and recovery.
A hologram is a piece extracted from the whole, but that still contains the whole. To attempt to pull out a part (either addiction or recovery) from the whole results in extracting a hologram (the full thing), not a mere “part”. Although what is pulled out is pulled out as separate, it contains both addiction and recovery.
Even more strange, recovery and addiction are mutually compatible as occurring together, because they are different aspects of one whole. Each is a mere “part”. But in this case of our field specifically, each mere piece contains the entirety, not just the part, or a part – but each piece contains both the parts and the whole.
So, consider the statement “I’m in recovery when I say I’m in recovery.” First, I will handle that statement as true, and then I will handle that statement as false. And even these evaluations (true, false) are partial reflections of a whole.
So, let’s examine the statement, “I’m in recovery when I say I’m in recovery”.
- It is true by principle because no one has access to the essence of the person’s person who is making the statement, or to their phenomenological experience, in order to claim otherwise.
(On the flip side, there are components of self we don’t have access to within and concerning ourselves. That is to say, seeing one’s self accurately (to say nothing of fully) is an undoable puzzle.
- It is true by example of the moment of clarity that happens to occur at a moment, such as the height of the illness.
What if a person at the height of their active illness has a moment of clarity and says so, and affirms their recovery in that moment?
- It is true by exploration of what comes before the moment of clarity.
What was the pre-clarity content and process? Worded differently, what was the recovery priming of the precovery phase? Why call that location, time, and material “precovery?” Isn’t splitting the precovery portion off from recovery per-se somewhat artificial?
And so let’s examine the statement “I’m in recovery when I say I’m in recovery” again.
- It is false by the same principle because the totality of the whole is still present.
That is to say, the addiction illness ego state in its most distorted form might be making the truth claim “I’m in recovery” when the claim is false. And it might be false even in their own estimation. (Ironically, even if it were false in their own estimation, on the grounds of point # 1. above, and out of respect for the person and that principle, we would still perhaps not disqualify the claim).
- It is false by example of the return to symptoms that comes before the return to drinking.
What (prodromal) signs and symptoms precede a return to full active illness – including return to a dynamic or pattern of old thoughts, feelings, attitudes, behaviors, personality function, and perhaps drinking or certain levels of drinking? (Read correctly, that question neither presupposes nor precludes sustained abstinence.)
- It is false by exploration of the process of a long, slow return to a lessening or lack of clarity before the moment of returning to drinking.
How far back in time do we need to look to find unstable sobriety, unstable psychosocial function, mere stasis, other problem-related prodromal material, or healthier recovery function?
2. The objective/subjective split error. Quantification (numeric data, etc.) is merely a representation of a thing through objective methods. By contrast, qualitative experience, and transfer of that experience through some means, is a source of information. (Subjective aspects of individual personal consciousness are called “qualia”).

Is a piece of music a composer creates the sheet music (an objective representation), or what the audience hears (a subjective experience)? Neither. The composed piece is in the mind of the composer and is accessible to no one. So here is a question: which of the two (objective or subjective) are the thing? And here is another question: if one assembles the objective and the subjective into one whole, is that the thing? No. It is not.
3. The nothing. “The nothing” can be important or helpful in a several ways. One way to help find a thing, identify a thing, notice its properties, or define a thing is to start instead with nothing – to start with what is beyond or past the edge of the thing, and therefore the space or “nothing” beyond the thing.

- What is “no addiction?” Does “no addiction” ever really come about during “recovery”? What is “no recovery?” Does “no recovery” really always persist during active addiction? Does “no recovery” always persist as-is before a moment of clarity? Is that even a thing? Thus, have we perhaps found recovery orphans?
- What is “no substance use disorder?” Here are some examples of what are called “diagnostic orphans”:
- During the many years we used the fourth edition of the diagnostic and statistical manual of mental disorders (DSM-IV) a “Substance Dependence” diagnosis required that a person fit at least 3 of the 7 criteria for substance dependence. Sometimes we would determine a person only met 2, or only 1. Those were “diagnostic orphans”.
- Another example is that sometimes we would determine that a person was worse off than the “substance abuse” criteria (above that threshold), but did not meet any of the worse “dependence” criteria (below that threshold). They were in a space between those two categories, belonging to neither. Those were also “diagnostic orphans”.
- Now we use the fifth edition, known as the DSM-5. Currently, to have a substance use disorder, a person must have 2 or more of the 11 criteria. But what if they have only 1? That person is a “diagnostic orphan”.
4. The person of the researcher. The questioner is placed in the question. Inside the question.
Recovery Orphans
Notes in Reaction to “The Myth of Matter”.
- When one views the ocean from 30,000 feet above the surface, the ocean appears flat, and the thing looks solid.

2. When viewed from a closer position, one notices waves that often appear in a pattern.

3. If one views the ocean from an even closer position, one notices foam atop the waves, and the presence of broken-off free-floating particles.

4. When the ocean is viewed from a very zoomed-in quantum level, there is more space than material.
References
Heidegger, M. (1927). What Is Metaphysics?
Wright, R. & Davies, P. The Myth of Matter. The Wright Show: MeaningofLife.tv, YouTube.
Suggested Reading
Coon, B. (2019). Addiction and the Stages of Healing. recoveryreview.blog/category/stages-of-healing
James L.(2016). Carl Jung and Alcoholics Anonymous: is a Theistic Psychopathology Feasible? Acta Psychopathol. 2:1.
Ortega y’ Gassett, J. (1927). Revolt of the Masses. W. W. Norton.
Rubianes, M, Muñoz, F, Casado, P, et al. (2020). Am I the Same Person Across My Life Span? An event‐related brain potentials study of the temporal perspective in self identity. Psychophysiology. 58:313692. https://doi.org/10.1111/psyp.13692
Thomas, C. (2013). Ten Lessons in Theory: An Introduction to Theoretical Writing. Bloomsbury: NY.
White, W. (2001). “The Rhetoric of Recovery Advocacy: An Essay on the Power of Language.” williamwhitepapers.com
White, W. (2013). Precovery: And Then A Miracle Occurred. williamwhitepapers.com
Previous Material (in order of release)
Brown, A. (2021). Reflections on Current Debates Regarding Recovery Definitions. recoveryreview.blog
Coon, B. (2021). Continuing “Very Heavy Drinking” and Also Meeting An Improved Definition of Recovery? recoveryreview.blog
Witkiewitz K, Wilson AD, Pearson MR, Roos CR, Swan JE, Votaw VR, Stein ER, Edwards KA, Tonigan JS, Hallgren KA, Montes KS, Maisto SA, Tucker JA. A Bridge to Nowhere: Resistance to the Possibility of Some Heavy Drinking During Recovery and the Potential Public Health Implications. J Addict Med. 2021 Feb 10. doi: 10.1097/ADM.0000000000000796. Epub ahead of print. PMID: 33577228.
Kelly JF, Bergman BG. A Bridge Too Far: Individuals With Regular and Increasing Very Heavy Alcohol Consumption Cannot be Considered as Maintaining “Recovery” Due to Toxicity and Intoxication-related Risks. J Addict Med. 2020 Oct 14. doi: 10.1097/ADM.0000000000000759. Epub ahead of print. PMID: 33060467.
Witkiewitz K, Wilson AD, Roos CR, Swan JE, Votaw VR, Stein ER, Pearson MR, Edwards KA, Tonigan JS, Hallgren KA, Montes KS, Maisto SA, Tucker JA. Can Individuals With Alcohol Use Disorder Sustain Non-abstinent Recovery? Non-abstinent Outcomes 10 Years After Alcohol Use Disorder Treatment. J Addict Med. 2020 Oct 14. doi: 10.1097/ADM.0000000000000760. Epub ahead of print. PMID: 33060466
Acknowledgement
I would like to thank Joe Najdzion for comments on a pervious version of this writing.
I’ve been involved in some recent discussions about addiction as a disease and the role of experiences like trauma.
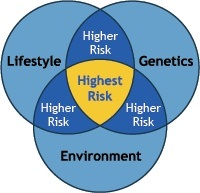
A few years ago I had the pleasure of seeing Dr. Jehannine Austin discuss how she approaches genetic counseling around psychiatric disorders and addiction. She doesn’t answer all the questions around the etiology of addiction (who can, really?), but she offers a very helpful frame for thinking about genetics, environmental risk factors, and protective factors. It also helps illuminate the role of recovery capital and social determinants of health.
Fortunately, her talk was recorded. The most salient parts are from 12:15 to 20:30.