

We only keep what we have by giving it away.
Altruism helps the giver. It’s at the heart of mutual aid and lived experience recovery organisations. This study from a few years back explores some of the issues in family recovery groups.
The researchers in this Finnish research looked at communication and support in Al-Anon groups, a 12-step mutual aid network for family and friends of those with alcohol use disorders. In Finland, 97% of Al-Anon members are female and three quarters are partners of problem drinkers. The academics conducted the research through questionnaires (169) and 20 interviews. In the survey they focussed on two questions:
- What elements of supportive communication are viewed as important?
- Why are they important?
Four themes came out of the questionnaires that were explored in the interviews:
- atmosphere
- sharing
- other group members
- others’ experience
What insights did the researchers get? Well they found that the feelings of ‘otherness’ caused by being in a family suffering with a loved one’s alcohol problems were addressed by being part of a support network where the positive community aspects of Al-Anon came into play. It was important to members that there was parity between members which helped with feelings of inferiority. In addition the taboo and stigmatised nature of alcohol use disorder in society meant that there could often be few ways to seek support, but Al-Anon provided it.
Sharing experience was key to healing. Storytelling allows the processing of information but sharing aloud also lets folk analyse feelings and ‘normalise’ difficult experiences. Our narratives are powerful things.
Ultimately the findings underpin an established truth; that, ‘the good of others is the good of oneself,’ a theme that must underpin effectiveness in all the mutual aid groups. The author conclude that the groups give permission for members to ask for help. By helping others, they themselves benefit. There is a functional role created by being a member; you can become and feel useful. Finally, there is the teaching that the only person you can change is yourself, and that is seen as empowering.
This is an study likely to be relevant elsewhere. It takes communication as a theme and explores its agency in Al-Anon groups, identifying and highlighting how human contact and storytelling, ancient and enduring elements of humanity, make practical differences to the lives of families suffering from alcohol use disorder. There is evidence here of the easing of stigma and of the building of self-esteem and empowerment.
There is some evidence that altruism is in some part genetic, but there’s something about warmth, concern and gracious consideration in this paper that makes me want to shy away from a reductionist, scientific explanation. I think the support given to help individuals and families suffering from alcohol use disorders or other drug addiction comes, at least in part, from love.
Continue the discussion on Twitter @DocDavidM
This is an updated version of a previously published blog
In their 2020 Commentary published in The Journal of Addiction Medicine (a journal of the American Society of Addiction Medicine aka ASAM), Kelly and Bergman state that:
“Individuals with regular and increasing very heavy alcohol consumption cannot be considered as maintaining ‘recovery’ due to toxicity and intoxication-related risks”.
Why did they publish a commentary about recovery and very heavy drinking being incompatible?
The commentary by Kelly and Bergman is their response to an article published earlier in 2020 in the same journal. It’s an article by Witkiewitz and others titled, “Can Individuals With Alcohol Use Disorder Sustain Non-abstinent Recovery? Non-abstinent Outcomes 10 years After Alcohol Use Disorder Treamtent.” In their article Witkiewitz and colleagues state,
“Nonabstinent AUD recovery is possible and is sustainable for up to 10 years after treatment. The current findings align with recent proposals to move beyond relying on alcohol consumption as a central defining feature of AUD recovery.”
Among other points, Kelly and Bergman note:
- A recovery definition should not entirely remove abstinence from alcohol use from the list of all recovery indicators
- Level of functioning regardless of amount of drinking should not become the sole indicator of the presence and level of recovery, as the Witkiewitz paper asserts.
- Classifying someone as “in recovery” should include consideration of “potential collateral damage to close significant others” as a factor.
- They go on to say that classifying someone continuing with ongoing very heavy drinking as “in recovery” would seemingly ignore the information close significant others could provide about the person’s level of function
- Those who are abstinent, but still struggling in psychosocial function per the Witkiewitz et. al. recovery definition, would be excluded by that definition from qualifying as “in recovery”.
- They go on to say this ironic and unintended consequence of a psychosocial function only recovery definition would promote stigmatization of the abstinent who are experiencing psychosocial struggles.
It looks to me like this is a full-blown open discussion of a recovery definition by academic researchers in the top peer-reviewed literature. I don’t think the discussion is over with, and it should be fascinating.
I could say a lot of things about a recovery definition that ignores the presence of drinking and that even ignores drinking at the level of very heavy drinking. And I could say a lot of things about the Kelly and Bergman response. For now, however, I’ll go a different direction and make some comments of my own that apply to the topic overall:
- I wish Kelly and Bergman would simply say “damage” or “additional damage” instead of “collateral damage” when describing the mental and emotional trauma experienced by those in the home, caused by someone who continues to drink. To me, “collateral” makes family members sound peripheral rather than sound like people.
- The Dry Drunk Syndrome can be terrifying for everyone experiencing it – drinker and family members alike.
- Symptom suppression is not enough. Recovery must be in the “do-direction”.
- Very heavy drinking is a danger to self and others.
- It’s interesting to see a recovery definition that seems to come from the perspective of research data alone and removed from clinical experience and lived experience.
- If we are coming at this from a clinical perspective, I wish we would include a focus on prognosis. That is to say, how do we expect the person to do? Or, “Are people getting better, or not?” To me, that is the central question.
- For example, if we are dying now or later from continuing cigarette smoking while drinking nothing, or drinking less, or showing improved psychosocial function, while meeting a new and improved recovery definition, while we continue our very heavy drinking, are we content with that?
For those that are interested, I’ll note that the Kelly and Bergman commentary has already produced a formal and published letter to the editor from Witkiewitz and colleagues. All three references are down below.
I might post more on this down the road.
References
Kelly JF, Bergman BG. A Bridge Too Far: Individuals With Regular and Increasing Very Heavy Alcohol Consumption Cannot be Considered as Maintaining “Recovery” Due to Toxicity and Intoxication-related Risks. J Addict Med. 2020 Oct 14. doi: 10.1097/ADM.0000000000000759. Epub ahead of print. PMID: 33060467.
Witkiewitz K, Wilson AD, Roos CR, Swan JE, Votaw VR, Stein ER, Pearson MR, Edwards KA, Tonigan JS, Hallgren KA, Montes KS, Maisto SA, Tucker JA. Can Individuals With Alcohol Use Disorder Sustain Non-abstinent Recovery? Non-abstinent Outcomes 10 Years After Alcohol Use Disorder Treatment. J Addict Med. 2020 Oct 14. doi: 10.1097/ADM.0000000000000760. Epub ahead of print. PMID: 33060466.
Witkiewitz K, Wilson AD, Pearson MR, Roos CR, Swan JE, Votaw VR, Stein ER, Edwards KA, Tonigan JS, Hallgren KA, Montes KS, Maisto SA, Tucker JA. A Bridge to Nowhere: Resistance to the Possibility of Some Heavy Drinking During Recovery and the Potential Public Health Implications. J Addict Med. 2021 Feb 10. doi: 10.1097/ADM.0000000000000796. Epub ahead of print. PMID: 33577228.

Join us on Monday, April 12th, at 1:00 p.m. ET for the new 2021-2022 Strategic Plan presentation.
Board President Bill Greer and Executive Director Mark Ruth will lead the discussion, sharing information on SMART Recovery’s new plan that includes:
- Growing and strengthening our volunteer base
- Developing our organizational culture, structure, and leadership
- Strengthening our financial resources
- Raising awareness, use, and support for SMART Recovery
The Zoom event is free with registration. The Zoom link will be emailed to you a few days before event.
We hope to see you there!
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!
Honor Your Treatment Court Heroes
Nominations open for national awards through April 30
Tell us about your treatment court heroes! Nominations are open now for national awards honoring outstanding treatment court professionals and teams. Awards are presented at RISE21, August 15-18 in National Harbor, Maryland!
Don’t delay, the deadline to submit your nomination is April 30.
Stanley Goldstein Treatment Court Hall of Fame
The highest honor in the treatment court field, this honor recognizes practitioners with unmatched contribution to the treatment court movement.
This award recognizes courts showing leadership to improve services across diverse populations, eliminate cultural disparities and ensure equity and inclusion in the court program.
This award recognizes outstanding DWI court practitioners or teams saving countless lives by advancing the nation’s DWI court movement.
Juvenile and Family Treatment Court Leadership Award
This award honors practitioners, teams, or organizations delivering outstanding service to families and/or juveniles in the justice system.
The post Nominations Open for NADCP National Awards appeared first on NADCP.org.

By: Dona Dmitrovic, Director, Center for Substance Abuse Prevention
In a world filled with a seemingly endless number of troubling headlines, it seems that everyone is looking for a bit of good news these days. And here it is: Underage drinking and substance misuse prevention is making an impact across the country!
According to SAMHSA’s National Survey on Drug Use and Health (NSDUH), instances of any alcohol use by individuals under age 21 have decreased since 2002. And between 2002 and 2019, current drinking by 12- to 20-year-olds declined from 29 percent to 19 percent.
While alcohol use by underage people has decreased since 2002, the decrease has been greater for underage males than for females. In 2019, more girls than boys reported past-month alcohol use. This highlights that while prevention is working, new challenges are emerging that require us to adjust attention and our strategies. And one of the biggest new challenges facing underage drinking prevention right now is the COVID-19 pandemic.
Since March 2020, young people have had to navigate disruptions in education, their social networks, and the disproportionate impact the pandemic has had on communities of color. As prevention professionals, we know that these are risk factors that can lead young people to start using and misusing substances. In fact, the CDC found that 1 in 4 young people ages 18 to 24 started or increased substance use in the past 30 days to cope with stress associated with COVID-19. Our prevention work needs to adapt to the new landscape. Fortunately, federal resources are rising to the occasion and providing communities with tools they can use even during the pandemic to promote prevention.
SAMHSA’s Center for Substance Abuse Prevention offers programs and resources to help communities tackle the impact of alcohol and other substances among youth and young adults. A key resource is the Communities Talk to Prevent Underage Drinking initiative, which launched its eighth round on February 4 and has an impressive track record of connecting communities to uncover and work through specific issues they are facing together.
Keeping disruptions to the prevention landscape in mind, this round of Communities Talk emphasizes activities that account for social distancing guidelines and changes in how individuals, families, and communities interact. By making these adjustments, we can maintain our commitment to underage drinking prevention while responding to new challenges in our communities. This is how we ensure Communities Talk 2021 continues to mobilize communities to raise awareness and implement evidence-based strategies to mitigate alcohol’s negative effects on young people. It also ensures prevention professionals understand the value of using Communities Talk as a tool to address mental health challenges created by the COVID-19 pandemic that we know can lead to unhealthy coping habits, such as alcohol use by young people.
I invite you to see for yourself the incredible prevention work communities have done in 2019 by reading success stories that communities have shared with us. These stories illustrate the inspirational events they have hosted that contributed to reduced rates of underage drinking in all 50 states and 6 U.S. territories. In 2021, we know communities will leverage this initiative to create new and inspiring ways to advance prevention.
SAMHSA offers a variety of other materials and resources communities can use, including many that combine personal stories with data to make prevention strategies attainable:
- The Sound of Your Voice –public service announcement and parent guide show the consequences of underage drinking that young adults transitioning to college often experience, as well as the vital role that parents can play in determining whether a young person decides to drink while underage.
- The “Talk. They Hear You.” national media campaign aims to reduce underage drinking and substance misuse among youth under the age of 21 by providing parents and caregivers with information and resources they need to talk about alcohol and other drug use with their children early.
- SAMHSA’s Substance Misuse Prevention for Young Adults guide supports health care providers, systems, and communities seeking to prevent substance misuse among young adults.
- The College Drinking: Prevention Perspectives two-part video series shows how underage drinking prevention strategies are implemented on college campuses: 1) “Lessons Learned at Frostburg State University” and 2) “Embracing Culture and Context to Prevent Underage Drinking.”
- The Quick Start Planning Guide includes everything community-based organizations need to know to begin organizing a results-oriented underage drinking prevention activity. The guide includes detailed steps for planning an activity, promotional tips using traditional and social media, ideas for sharing your work, and commonly asked questions about how to use a Communities Talk stipend
To learn more about the many ways SAMHSA supports underage drinking prevention both nationally and locally, visit www.stopalcoholabuse.gov. This is also a great place to learn about Communities Talk and take the first step in using this initiative to support underage drinking prevention in your community.
We are proud of the progress we’ve made so far, and we are excited to see what the future of prevention holds for our nation. Thank you for your continued support in reducing underage drinking and substance misuse.
Prevention works!
Now Accepting Submissions to the Journal for Advancing Justice Vol. IV
NADCP is pleased to call for submissions to the next volume of our peer-reviewed Journal for Advancing Justice: “Justice Reform: Achieving Evidence-Based Practices in Community Corrections to Promote Recovery.” This issue is supported by a grant from the Office of National Drug Control Policy, Executive Office of the President. The United States and other nations are at a major crossroads. As communities and advocates continue to call for change at the federal, state, and local levels, justice reforms are taking hold at an unprecedented pace. While many reforms are clearly necessary and well-intentioned, it has become more critical than ever that law, policy, and practice shifts be grounded in rigorous scientific research. If we are to ensure lasting positive change, we must conduct research in critical areas that have not received adequate attention, as well as build on existing findings from community-based interventions that have been proven to work, such as treatment courts, law enforcement deflection initiatives, prosecutor-led diversion programs, and other alternatives to incarceration.
We are looking for original research reports and research-based review articles or meta-analyses to address priority topics such as:
- Collaborative strategies for the treatment and justice systems to coordinate care effectively for high-risk and high-need participants
- Effective parameters for community supervision practices, such as home or employment visits, GPS monitoring, house arrest, remote check-ins, drug and alcohol testing, and application of core correctional practices
- Optimum program lengths and dosages of services based on participant risk and need
- Methods for enhancing or building on recovery capital for participants
- Effective roles and functions of peer recovery support specialists or peer mentors
- Effective harm reduction strategies and how to apply these in the context of community corrections programs
- The impact of drug decriminalization or legalization on applications of best practices
- Trainings or interventions demonstrated to enhance equity and inclusion for various racial, ethnic, or other cultural groups
- Self-care and wellness strategies for justice professionals to enhance workforce development, including strategies for coping with loss and grief
Click here to learn more and submit.
The post Now Accepting Submissions to the Journal for Advancing Justice Vol. IV appeared first on NADCP.org.
Those who cannot remember the past are condemned to repeat it.” – George Santayana
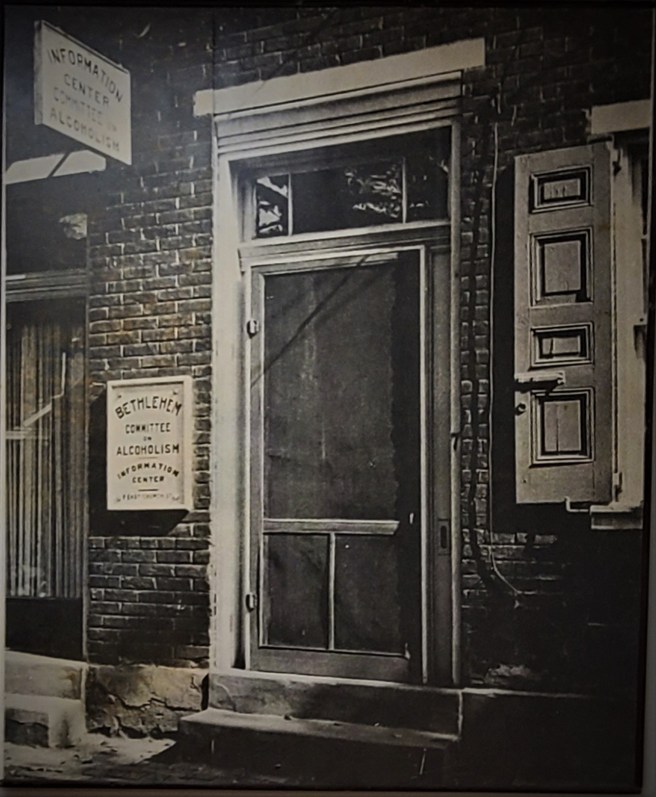
The other day I was on a zoom call and I could see a poster of local recovery history behind one of the persons I was talking to. I asked about it, and he told me he had stumbled on the poster when a local agency was cleaning out a condemned building. They were going to throw it out. He salvaged it for a local recovery community center because he was in the right place at the right time. I gave him a brief history of what I recalled about the place and the historical significance it held. It was one of the first alcoholism councils in the nation, the Bethlehem Council on Alcoholism. It was started in in 1950 and was renamed before being disbanded in the 1990s. As I got into recovery in the mid-1980s, I knew people who had worked there and how it related to a lot of the local service system.
They were our local pioneers, and it linked back to 1944 and Marty Mann and National Committee for Education on Alcoholism. The very notion that Alcoholism was a disease, and to educate the public on the fact that alcoholism is not a moral failing was a radical concept. I thought back to some of the people I had the opportunity to meet in my early recovery and their significant life contributions to these early efforts. I got help through one of the organizations that came out of this era and later ran it. Their efforts before I was born helped save my life. They developed services for “our people” because no one else cared, a theme that repeats through history as Bill White wrote about.
So what are we doing to lift young leaders onto our own shoulders? What will they know about how we got here or how to use that knowledge to make educated decisions about where to go next?
We have done a very poor job of transferring our own history on any level, local, state or nationally. We do not transfer knowledge about what we have learned along the way in any organized fashion. As a system, we do next to nothing to groom young leaders with heart for the work to carry the mission forward. We do almost no succession planning. We do not groom younger leaders into roles in which they learn in depth about our systems, our history and our successes and failures. We fail to understand that people with lived recovery experience are the backbone of our care system and we must include them as vital to preparing for future needs.
Forgetting our past and failing to prepare for our future.
Teaching about our collective failures could well save a lot of future pain and suffering so they learn from our mistakes without having to repeat them. Without the life work of Bill White, we would not even have a place to look to go to and examine our history and benefit from the wisdom of the people who have forged ahead of us. His interviews, monographs and papers provide context and insights that would otherwise be lost history. The truth however is that most of our young leaders do not even know of his work or the historic struggles they overcame to realize even the limited successes we see in front of us today.
And now we face an ever-deepening workforce crisis in the SUD care system. We know it is there, SAMSHA recently completed a report showing we need major recruitment across all Behavioral Health Sectors just to stay even with pre-COVID care demand. A decade ago, our annual workforce turnover rate was between 19% and 50%. Since then, annual total US workforce turnover has increased 88%. This Behavioral health study, published in 2020 suggested a 45% annual turnover rate based on its sample. HRSA is going to be doing an additional study.
We are collectively failing in recruitment, retention, and succession planning. Even as treatment and recovery services have never been more needed and institutional knowledge is walking out of doors across our care system.
We are failing in our field stewardship responsibilities to mentor and develop new recovery leaders. Well respected, and deeply contributive organizations whither and fail when new leaders were not properly groomed and steeped in our history or trained to understand the nuances of the work. They do not know what they do not know. A form of Institutional amnesia. According to this article, less than half of our Behavioral Health Organizations have any kind of succession planning in place. That we fail to try to develop new leaders to understand the challenges we faced, and the value of historic knowledge is nothing short of a crime.
Most of the perennial studies I have seen over the last few decades raise remarkably similar points about the barriers. It is time to move to solutions. Perhaps we can move more resources into workforce retention and leadership development. We can start with the recognition that people in recovery are the foundation of the SUD workforce. We can build recovery capital by investing in leadership programs that mentor new recovery leaders in every state across the nation. If we do this, we will invest in those with heart, those who stick and stay across an entire career.
Some questions to consider:
- What is the history that led to your local organization being founded?
- What were the visions and motivating elements that drove your historic leaders to do what they did?
- Did those pioneers make mistakes we can learn from so we can avoid repeating them?
- How does your organization groom potential leaders to understand and build upon foundational work?
- Is your organizational history even written down – are people aware of their own organizational history?
- How can new leaders effectively navigate organizational, and systems change challenges without knowledge of where the hidden reefs and sandbars are?
- What resources do we devote nationally or at the state level for workforce succession and leadership development?
- Why do we not invest in field leadership development?
- Are we always in such a perpetual crisis that we continually postpone forward focus on succession planning?
- If you run an organization, what would happen if you got hit by a bus tomorrow?
In short, our entire substance use care workforce dynamic can be summed up under the perspective that our futures are inseparably entwined, and we are not investing in it in meaningful ways. We will sink or swim together and unless we put a lot more effort in, my sense is we shall sink. Our future is a collectively bound. We fail when we forget the past and do little to prepare for the future. Let’s do the former rather than the latter.
If there is anything more important that preparing our to sustaining efforts to expand recovery than steeping new leaders in our history and helping them prepare for our future, I do not know what it is.
What is needed:
- Recovery leadership academies in every state, run by and for the recovery community to ensure that the work of recovery strengthens community recovery capital.
- A focus on understanding that people with lived experience are most likely to be retained over the long term so they are the vital element to prepare for the future.
- Recovery oriented mentorship processes that build resources within regional communities
- Recovery oriented mentoring processes that develop new leaders that emphasize our shared history and developing skill sets to prepare for future challenges.
- Strengthening of career ladders that identifies younger talent and provide the means for coordinated development.
- Efforts to remove barriers to employment, such as historic legal histories that can prevent people from getting into the workforce and obtaining employment, even many decades after they are in recovery.
If any readers in policy positions who want to focus work on this issue or get some of us formerly young leaders who still have heart for the work to put effort here, please count me in. It is one of the things I wish to devote my remaining time on. I want to be part of the solution.
I owe it to those whose shoulders I am perched on, I suspect I am not alone.
The best time to do this was twenty years ago, the second-best time is right now.
Additional Reading links:
Leadership in Addiction Treatment: The Coming Crisis – William L. White (2002) – Link HERE
Calling a New Generation of Leaders – William L. White and Lonnetta Albright (2006) – Link HERE
Staff Turnover in Addiction Treatment: Toward Science-Based Answers to Critical Questions – William L. White, MA and Bryan R. Garner, PhD (2011) – Link HERE
Time to BLOOM — Grow your Recovery Support Network!

If it’s something weird and it don’t look good
Who ya gonna call?
Ghost Busters!
Well…not exactly. Who are you going to call in moments of need throughout your recovery? Who will you call when things are going well? A strong support network is essential to successful long-term recovery. It is important to surround yourself with individuals that understand your situation and support your recovery.
At the beginning of your recovery, you might find that your approach to friendships and relationships has changed for you. You also probably had to leave some of the relationships from your days of active addiction behind you. This doesn’t mean that you’re destined to a life of less connection — no one recovers alone. Learning how to build your network takes time, but here are some helpful hints to get you started:
Actively Attend 12-Step Program Meetings
Many Alcoholics Anonymous and Narcotics Anonymous meetings are currently virtual, but that doesn’t mean you can’t still actively participate in the 12-Step Communities. So long as you have a desire to pursue sobriety, you are welcome in the rooms of AA and NA.
If you’re new to the sphere of 12-Step meetings, stay after and talk to some of the others in attendance, whether that’s in person or in the chat of the Zoom meeting. Those in recovery are almost always eager to help others, and remember—they were once new, just like you. Much like your recovery, sometimes the first step of reaching out when building connections is the hardest part, but it does get easier with practice!
Find a Sponsor
You must find someone with experience and empathy to assist you as you work through the 12-Steps. A sponsor is someone that you feel comfortable being completely honest and open with. As another individual who has worked through the same disease as you, they should understand you and be close to you in your recovery in a way that few others could be.
This is the person who can encourage you when times are tough, and guide you when you feel lost. Those moments will present themselves throughout your recovery journey, and it is important to seek the mentorship and connection of a sponsor in your fellowship. Continue on with attending meetings and connect with as many individuals as possible. As you build relationships, you will know when you’ve found the person who is the right fit.
Reconnect and Rebuild Healthy Relationships
Finally, encourage your family and friends to educate themselves in regard to the disease of Substance Use Disorder. If you are fortunate enough to have maintained a relationship with your loved ones after your time in active use, turn your attention toward improving those relationships through your program of recovery. If you are not in contact with loved ones due to mistakes made during active use, work with your sponsor and in your program on making amends to those individuals you might have wronged.
It may take some education, time, and consistency, but surrounding yourself with your loved ones who want the best for you in your recovery can be an incredibly valuable source of support in your network. Your loved ones can find resources to learn more about your recovery at https://al-anon.org/ or https://www.nar-anon.org/.
***
For more information, resources, and encouragement, “like” the Fellowship Hall Facebook page and follow us on Instagram at @FellowshipHallNC.
About Fellowship Hall
Fellowship Hall is a 99-bed, private, not-for-profit alcohol and drug treatment center located on 120 tranquil acres in Greensboro, N.C. We provide treatment and evidence-based programs built upon the Twelve-Step model of recovery. We have been accredited by The Joint Commission since 1974 as a specialty hospital and are a member of the National Association of Addiction Treatment Providers. We are committed to providing exceptional, compassionate care to every individual we serve.

I would tell them straight, recovery does not happen in isolation
Recovery group member
We know mutual aid works to help people with substance use disorders achieve their goals. The recent Cochrane Review[1], which analysed the evidence for Alcoholics Anonymous reported pretty impressive results. John F Kelly, Keith Humphreys and Marica Ferri “determined that AA was nearly always found to be more effective than psychotherapy in achieving abstinence. In addition, most studies showed that AA participation lowered health care costs.’[2]
Although the focus of the research has been more on AA than other types of mutual aid, Humphreys said that their review was ‘certainly suggestive that these methods work for people who use heroin or cocaine’. In fact, these days, in my practice, it’s much more common to see people with problematic poly-drug use, so it would help to know more about the range of supports available.
So, we know that mutual aid works to help people achieve their goals, but how much do we know about how it works? In his 2008 review[3], Rudolph Moos identified ten key ‘ingredients’ at the heart of the process in 12-step groups.
- Bonding
- Direction
- Structure
- Observation and imitation of norms and role-models
- Expectation of positive and negative consequences
- Involvement in protective activities
- Effective rewards
- Identification of high risk situations and stressors
- Building self efficacy/confidence
- Developing coping skills
So, it looks as if we know quite a bit about how it works too, but we are still learning new things.
Some of this new learning was captured in a recently published study[4] from the UK. Hannah Rettie, Lee Hogan and Miles Cox wanted to know if such processes might also apply in non-12-step groups and whether there might be anything else relevant that wasn’t on the above list. They had the sensible notion to ask the people who had experience of such groups how important they felt these components were.
Using social media, flyers and active recruitments through the groups, they attracted 151 participants from 30 groups, including but not limited to, 12-step, SMART Recovery and non-structured lived experience community groups. Participants had to be alcohol or drug free, with a previous history of dependence and regular attendees. On average the subjects had been members for more than two years and had a mean age of just over 42 years. Thirty percent had previously had an alcohol problem, 20% a drugs problem and the rest had used both alcohol and drugs problematically.
They asked the participants to think about their group and to score how important each ingredient on the list was to them and how much that component was represented in the group they were a member of. They were also asked a couple of open questions. The researchers divided one of the ingredients (no. 4) into two – ‘presence of role models’ and ‘following a sober lifestyle’ and added another ingredient ‘giving back to others’.
They teased out five pertinent themes from the open-ended questions:
- Perspective taking: e.g., getting a new angle on a problem through discussion with others
- Being connected to others: e.g., strong bonds, reciprocal support, not doing it alone
- Developing skills: e.g., coping skills, confidence, useful outside of the group too
- The value of group activities: e.g., replacing using and drinking time, hobbies and areas of interest
- A change in the self: e.g., from rock bottom to recovery, gaining hope, new lease of life
These themes were apparent in both 12-step and non-12-step groups.
Testing out the list of key components of recovery success, the researchers found that across the variety of groups, every ingredient was both offered by the group and rated highly by the group members. Interestingly ‘gaining rewards’ was not rated as highly as other factors. The type of group, length of time of membership and time in recovery did not influence the ratings.
The team updated the original table of important components of recovery groups to look like this:
- Bonding and support
- Goal direction
- Structure to follow
- Following a sober lifestyle
- Available role models
- Expectations of positive and negative consequences
- Involvement in protective activities
- Effective rewards
- Identifying high-risk situations
- Building self-confidence
- Developing coping skills
- Giving back
- Presence of like-minded individuals
- Developing self-awareness and reflection skills
Encouragingly, these findings suggest universal experiences in mutual aid and lived experience recovery organisations, though not whether these experiences translate into longer term quality of life and sobriety outcomes relating to type of support. It’s important to note that the authors acknowledge potential bias due to recruitment methods, so this might not in fact be applicable to all recovery groups, though it rings true. I did wonder if there was crossover in the sample, given that it’s possible to be a member of a 12-step group, a SMART Recovery group and an activity-focussed recovery group at the same time.
I like this research. I like the respect the researchers have for those with lived-experience (‘true experts’) – something that’s not universal. Mutual and and wider lived experience recovery organisation research is pretty rare in the UK. This really helps add to our understanding of what the important features in recovery groups are. It adds to our previous understanding. It also gives support to the ‘many pathways to recovery’ perspective.
Connection is at the heart of the recovery process. In my experience, many recovering people are members of more than one lived experience recovery organisation, including mutual aid. I believe that every extra recovery connection is likely to advance and support an individual’s recovery and help them flourish, and that we should be promoting and actively connecting service users to a diverse range of groups.
The researchers’ bottom line:
The current study provided support for Moos’ original components, and identified that these components are universal across a diverse range of recovery groups, and stable across time. The findings offer an in-depth, person-focused perspective into what makes recovery groups successful, utilising the voices of the true experts of addiction recovery groups.
Rettie, Hogan & Cox, 2021
Continue the discussion on Twitter: @DocDavidM
[1] Kelly JF, Humphreys K, Ferri M. Alcoholics Anonymous and other 12‐step programs for alcohol use disorder. Cochrane Database of Systematic Reviews 2020, Issue 3.
[2] https://med.stanford.edu/news/all-news/2020/03/alcoholics-anonymous-most-effective-path-to-alcohol-abstinence.html
[3] Moos RH. Active ingredients of substance use-focused self-help groups. Addiction. 2008 Mar;103(3):387-96.
[4] Hannah. C. Rettie, Lee. M. Hogan & W. Miles. Cox (2021): Identifying the Main Components of Substance-Related Addiction Recovery Groups, Substance Use & Misuse
Guest blog by Matt/M11106
On March 16, 2021, Robert Long was charged with killing 8 people, 6 of them Asian women, in Acworth and Atlanta, Georgia. SMART recognizes the deeply intertwined nature of the racism and misogyny that played a role in this tragedy. We mourn the loss of life and send our deepest condolences to the victims’ families, friends, and communities. We are taking this occasion to publish a post by the facilitator of our meeting on Sexual Maladaptive Behaviors.

An Open Letter to Men Who Struggle with Sexual Maladaptive Behaviors:
According to the Washington Post, Robert Long told police that he has “a sexual addiction” and the massage parlors and spas he targeted were “a temptation for him that he wanted to eliminate.” This tragedy has made me think of how SMART could have helped Long better manage his impulses. I believe SMART can help Long and any other man struggling with these thoughts and behaviors.
I wish that Long had attended some of our SMART meetings on sexual maladaptive behaviors. As it stands, he is charged with eight counts of murder, so it is too late for our meetings to help him and prevent the tragedy from occurring. But even in jail, a man might want to find a calmer mental state regarding his maladaptive behaviors.
If Long had attended, he might have shared that he wanted to remove temptation at massage parlors. He might have said he was struggling with shame around his sexual behaviors, as his roommates from rehab have said.
In SMART, we often manage temptations by avoiding the situation, escaping the urge, or substituting healthy activities. There will always be temptations for us, but we can learn how to choose behaviors so that the temptations that are problems for us can be parts of other people’s lives, rather than our own.
We often respond to shame with a SMART vocabulary exchange, like replacing the shame of being a bad person with regret for your past behaviors. That exchange may make it easier to plan and achieve new behavior in the future.
We’d also question the bad-person description. We might reframe it as “my actions were not consistent with my beliefs”. Then we can ask: Do you believe these beliefs that you mentioned, which you may have learned from other people? Do you want to change your beliefs? Do you want to change your actions?
The men who want to change their actions in this area often begin by saying “I don’t want to treat women as objects.” Some men find it helpful to remember that the women they see are somebody’s mother, somebody’s daughter, somebody’s sister, somebody’s wife. Some men find the empathy to say, “I want to respect these women and their goals.”
In Acworth, Xiaoje Tan owned the Asian massage parlor and told her daughter she wanted to retire. Delaina Yaun had just gotten off work and was getting a massage at the same time as her husband. In Atlanta, among the employees of Gold Spa, Hyun Grant dedicated her life to providing for her sons. Yong Ae Yue liked introducing friends to home-cooked Korean food and Korean karaoke.
Long’s violence robbed these women, and the other victims, of the opportunity to achieve their goals. But Long, and other men with SMBs, still have the option of pursuing paths that respect women, and to find a healthy way to integrate some sexual desires with the rest of their lives.
These are the sorts of topics that we discuss in our meetings on Sexual Maladaptive Behaviors. It is powerful to talk about them in a community of people going through their own recoveries from similar issues and working through the many SMART tools that can help.
The meetings are online on Sunday evenings, and are open to everyone. While I don’t expect that Long will be able to attend, I hope that you and any other people dealing with similar issues will join us.
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!