

Although COVID has changed many plans this year, we want you to know that you are not alone this holiday season. In keeping with our holiday traditions here at SMART Recovery, we are excited to once again offer our virtual annual New Year’s Eve Around-the-World event through SMART Recovery Online (SROL).
This nonstop meeting with hourly start times begins at 5:30 a.m. ET on December 31, 2020, and ends at 3:30 a.m. ET on January 1, 2021. Online meetings are laid back and fun with hourly themes selected by that meeting’s host.
A few of this year’s themes include:
- Holiday Triggers and Urges Awareness
- Trivia Around the World
- Recovery Music and Lyrics Chat
- Micro-Resolutions for 2021
- Looking Back, Looking Forward
- Relapse-Prevention, Warning Signs and What You Can Do to Recover From Them
- And more!
(See the full schedule at the bottom of this article or downloading this PDF.)
HOW TO PARTICIPATE: This event is completely free-of-charge. To participate, use your SMART Recovery Online (SROL) login credentials. You can create SROL credentials for free at www.smartrecovery.org/community.
Wishing you a safe, happy, and healthy New Year.
Meeting Schedule:
Download this printable PDF to see full schedule with host names.
- 5:30 a.m. ET – Meditation, Well-Being, and Self-Care
- 6:30 a.m. ET – Better Communication to Help Family Relationships
- 730 a.m. ET – SMART Recovery General Meeting
- 8:30 a.m. ET – Holiday Triggers and Urges Awareness
- 9:30 a.m. ET – SMART Games
- 10:30 a.m. ET – With every passing second you’re a new person: Rediscover, Redevelop, Recreate
- 11:30 a.m. ET – Creating Confidence Exercises with Eboni
- 12:30 p.m. ET – “We need to talk…”
- 1:30 p.m. ET – How I (personally) understand SMART Recovery
- 2:30 p.m. ET – What is your Fight Song?
- 3:30 p.m. ET – SMART Recovery General Meeting
- 4:30 p.m. ET – Trivia Around the World
- 5:30 p.m. ET – (Topic Pending)
- 6:30 p.m. ET – SMART Relationships
- 7:30 p.m. ET – What is Up with You on New Year’s Eve?
- 8:30 p.m. ET – SMART Recovery General Meeting
- 9:30 p.m. ET – Micro-Resolutions for 2021
- 10:30 p.m. ET – Recovery Music and Lyrics Chat
- 11:30 p.m. ET – Rule #32: Enjoy the Little Things – Learning to celebrate every victory
- 12:30 a.m. ET (Jan 1) – Looking back, looking forward
- 1:30 a.m. ET (Jan 1) – Relapse-Prevention, Warning Signs and What You Can Do to Recover From Them
- 2:30 a.m. ET (Jan 1) – How Blogging, Vlogging, Podcasting, Journaling, and Making Videos Can Help Your Recovery
RSVP on Facebook
Help us spread the news of our free, virtual event with your connections. RSVP to this event on Facebook and share it with friends and family.
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!

Those harm reduction initiatives are great. I would say ‘keep doing that’. But also give people the opportunity to get well because that mantra of ‘keep them alive, keep them alive’ isn’t good enough. As a person in long-term recovery, I see it as a lack of ambition. It’s disrespectful to assume I am not worthy of healing.
I shared a larger quote the other day that included this and it got some pushback from people who read it as dismissive of harm reduction or an expression of one-way-ism. I explained that I don’t read it that way at all.
At any rate, I read a press release about a recently published study and Annemarie’s words about “lack of ambition” came to mind.
The study focused on opioid agonist patients in Vancouver, BC. Here’s what the press release reports:
- There were 819 participants in the study.
- 53% tested positive for fentanyl despite being on opioid agonist treatments (OAT).
- Participants who tested positive for cannabis were 10% less likely to test positive for fentanyl.
The paper adds the following:
- All were receiving opioid agonist treatments in a community setting.
- More than 80% were receiving methadone
- 53.6% tested positive for cocaine
- 44.7% tested positive for methamphetamine
There are a few things that are a little confusing in the paper, but I believe they report:
- 66% tested positive for cannabis. 1
- People who tested positive for cannabis were more likely to test positive for benzos. 2
Those are the findings.
As with most things, there’s more than one way to understand the findings. Some might question the efficacy of the treatment, others might wonder if there are any psycho-social services provided, and others might wonder about the dosing. I think most people would view these as disappointing findings, particularly given BC’s status as a frequently cited North American leader on drug policy.
These researchers bring a different set of assumptions and reach a different set of conclusions.
- these patients are “supplementing their treatment” with street drugs
- reduced fentanyl use means reduced risk of OD
- the 10% lower rates of positive fentanyl tests among patients testing positive for cannabis is understood as “stabilizing”
- this underscores the need to better understand “the therapeutic potential of cannabinoids as adjunctive treatment”
- daily cannabis users were 21% more likely to be retained at 6 months, which is understood as “a beneficial link between high-intensity cannabis use and retention in treatment”
- this is in the context of a growing evidence-base “suggesting cannabis could have a stabilizing impact”
- “cannabis might have a role in addressing the overdose crisis”
What the study and press release don’t tell us:
- rates of benzo use among patients and, more specifically, those who test positive for cannabis
- rates of use for opioids other than fentanyl
- what are the retention rates in the programs these patients received services from?
- other kinds of treatment patients may be receiving
- patient satisfaction with their treatment, progress, and quality of life
- what other options are available to these patients
I have two reactions to this.
First, I can’t help but wonder if the researchers would find these outcomes attractive or promising for themselves or a loved one.
Stigma gets a lot of attention these days. We usually associate stigma with judgmental or punitive responses to to addiction. I believe that low expectations are a too frequently ignored manifestation of stigma. Personally, I believe these outcomes could only be considered good in the context of seeing these patients as hopeless or as an “other.”
Second, we hear a lot of calls to follow the science, for evidence-based treatment, and OAT as the gold standard of care, often to the point of delegitimizing other models.
This study and press release highlight the importance of asking “evidence-based for what?” Does the evidence-base address your goals and hopes for yourself of your loved one? When experts communicate the evidence-base to you, what hidden assumptions are embedded? 4
Continued evaluation of treatments is extremely important. We do not have any silver bullet treatments and need to accurately communicate the strengths weaknesses of each option, and explore how they align with their goals. Yes, OAT dramatically reduces OD, but retention rates are not great and the evidence-base does not speak to the goals of many patients. Yes, PHPs have outstanding outcomes, but many PHP elements are not available to most patients and coercion undoubtedly plays a role in the success of those programs.

It’s an unfortunate truth that any patient or family member should be very skeptical of anything they hear from treatment providers, advocates, researchers, and journalists. This isn’t to say everyone is untrustworthy or dishonest, but too many of us are focused on a relatively narrow set of concerns. A friend compared understanding addiction, recovery, & treatment to an 8 sided die and added that most practitioners, advocates, researchers, and journalists are focused on only one side of the die.
- See table 1, row 1. It looks like 66%, but the fact that the Ns for columns 2 and 3 don’t equal the N for column 1 is throwing me.
- It says “at baseline”, which doesn’t make sense to me, because this is just an observation of OAT patients over a period of time.
- This statement referred to a study on OAT improvements over a 10 year period with the implementation of a cascade of care model. They defined retention as ≥ two observations in a given calendar year at least three months apart where the participant reported being enrolled on OAT. Retention rates improved from 29.1% to 35.5%. They defined stabilization as no self-reported overdoses, no binge drug use and no fair/poor self-reported health due to drug use among participants retained in OAT in the calendar year. Stabilization rates improved from 10.1% to 17.1%.
- This is not specific to OAT. These questions should be applied to all information about treatment and outcomes, whether it’s residential, outpatient, OAT, or whatever.
Thanks to Brian Coon for his comments on this post.
 There is a famous quote – “Americans Will Always Do the Right Thing — After Exhausting All the Alternatives” often credited to Winston Churchill. I have been thinking about the quote as it relates to the narrative around deaths of despair and the erosion of social connections, hope and purpose. These deaths are often related to addiction, and addiction seems to be at the heart of so very much that ails us as a nation. To address deaths of despair related to addiction we must focus on developing community recovery capital as a primary intervention strategy.
There is a famous quote – “Americans Will Always Do the Right Thing — After Exhausting All the Alternatives” often credited to Winston Churchill. I have been thinking about the quote as it relates to the narrative around deaths of despair and the erosion of social connections, hope and purpose. These deaths are often related to addiction, and addiction seems to be at the heart of so very much that ails us as a nation. To address deaths of despair related to addiction we must focus on developing community recovery capital as a primary intervention strategy.
So what is community recovery capital? For a definition of Community recovery capital, I would refer readers to this 2008 paper by William White and William Cloud titled Recovery Capital: A Primer for Addictions Professionals. They define community recovery capital as encompassing community attitudes / policies / resources related to addiction and recovery that promote the resolution of alcohol and other drug problems. In short, developing community recovery capital strengthens civic engagement while providing participants hope and purpose.
This is exactly what we should wake up every day trying to increase across America right now.
This is because expanding recovery capital spreads recovery. Yes, recovery is contagious – it spreads. So “seeding” and nurturing recovery at the community level can offer broad benefit to the whole community. To understand how recovery can be contagious, I would refer readers to a paper by David Best and Alexandre B. Laudet titled The Potential of Recovery Capital. In that paper, they describe how “smoking cessation by a spouse decreased a person’s chances of smoking by 67%, while smoking cessation by a friend decreased the chances by 36%. The average risk of smoking at one degree of separation (i.e. smoking by a friend) was 61% higher, 29% higher at two degrees of separation and 11% higher at three degrees of separation.” This works for other addictions as well.
Pause and consider that expanding recovery in our communities has protective and preventative elements for the entire community. Additionally, broad, societal focus on expanding hope, connection and purpose within communities would be beneficial to changing the dynamic of our current addiction crisis by spreading recovery.
A huge problem is that as a society, we incorrectly conceptualized our addiction problem as an opioid epidemic (even as 90% of persons using opioids are using other addictive drugs). We are currently measuring “success” as the reduction of overdoses even as addicted persons continue to die from things other than overdose. In short, the wrong metric – reducing overdose deaths will end up having us miss the boat on effective strategies to save and restore lives and communities while keeping us stuck in tragic loss and the cycle of addiction.
It is important to change the narrative to one in which we educate our communities on the broad impact that recovery has and get our policymakers and philanthropic leaders to focus resources beyond our traditional care system (while still supporting care for acute service needs).
We cannot develop the resources and supports necessary to strengthen recovery within our communities if policymakers largely see things from a traditional acute care framework. We must change the narrative to focus on expanding recovery capital at the community level. The primary healing agent in healing addiction is community, lets focus resources there.
We must:
- Focus on long term recovery – 85% of people who get into long term recovery remain in recovery for life.
- Continue to reduce overdose rates, dead people cannot recover. Harm reduction efforts are key to keeping people alive, yet as multiple drug addiction is the norm, not the exception, the ultimate goal for addicted persons must be recovery.
- Not get trapped in narrow metrics. We have an addiction epidemic in which recovery is the probable outcome given the proper care and support for people who have substance use conditions.
- Most persons with addictions use multiple substances so whole person care is imperative with an emphasis on developing and sustaining resources within the community is key to saving lives and communities.
- The development of community recovery capitol must be funded as a primary objective, not as an afterthought.
We cannot simply hope it will happen without resources and sustained focus. This will require broad sustained effort across government and philanthropic institutions. Advocacy starts with us.
It is beyond time. Our communities are worth it.

In this essay I make two claims. My two claims will take the form of slightly changed versions of two borrowed sentences. (I will present the original versions of the two borrowed sentences later in the essay). I simply took the borrowed sentences and changed a few key words. In my changed version of each sentence, you will see in italics the words I inserted to replace certain words found in the original sentences.
Here are my two claims:
- For recovery advocacy, no consistent system of axioms whose theorems can be listed is capable of proving all truths about recovery.
- There will always be statements about natural recovery that are true but that are unprovable within the system. And recovery cannot demonstrate its own consistency.
By extension, then, I state that recovery itself is, in a manner of speaking, “false”, or “unprovable” – but useful anyway.
What is interesting is that the program of 12-step recovery is a total system, not just an “outcome”.
(By “total system” I mean to highlight at least two things. First, the 12-step version of recovery concerns the whole matter of one’s alignment to one’s self, others, and the world at levels including behavior, thoughts, values, priorities, and personal development over time. Secondly, not only is 12-step recovery focused on a wide scope of personal change, but it also provides and encourages development of a social structure within which one can undertake and live out the work itself, and one’s recovery.)
Criticism from Empiricism
Critics of traditional 12-step recovery criticize it on various grounds. Critics often assert that the most compelling arguments against it are those we find under simple scientific scrutiny.
That criticism is traditional. For thousands of years in the west, tools of verification have included formal logic, math, and structured observation. Later, the scientific method as we know it arose.
As a process, empiricism clears the air of superstition and false beliefs. Periodically, applying processes of logic, observation, or scientific study exposes some “facts” (that have long functioned as “received knowledge”) as actually nothing more or less than simply false. Examples include setting aside the notion of a flat earth, a solar system with the earth at the center, and so on.
On the tree of science1, the study of social systems is held to be the most spongy and most lacking of rigor. Or so it is claimed. After all, the real science inside the study of social groups is psychology. And of course, for psychology the more pure real science is biology. If one knows everything about biology, one will already have psychology. And for biology we all know the real science is chemistry. But chemistry is nothing more than applied physics; learn physics and you will have the essence of chemistry. Last and best of all is math itself – the pure content that is the essence of physics and core material of the scientific method. Math is most pure. Or so it is claimed.
For thousands of years in western philosophy it has been set forth that everything that is true: 1) must not be self-contradictory or internally inconsistent and 2) must be provable and subject to proof.
Certainly, math is best and most pure of all.
Math Is Not the Path
But interestingly, math itself is nothing but a model and under proper scrutiny math collapses in violation of itself and of our hopes. The quotation that follows expounds that fact and lists as numbers 1 and 2 (I added the numbers themselves for clarity) the two borrowed sentences I used to start this essay.
“Gödel’s incompleteness theorems are two theorems of mathematical logic that demonstrate the inherent limitations of every formal axiomatic system capable of modelling basic arithmetic. These results, published by Kurt Gödel in 1931, are important both in mathematical logic and in the philosophy of mathematics. The theorems are widely, but not universally, interpreted as showing that Hilbert’s program to find a complete and consistent set of axioms for all mathematics is impossible.
The first incompleteness theorem states that no consistent system of axioms whose theorems can be listed by an effective procedure (i.e., an algorithm) is capable of proving all truths about the arithmetic of natural numbers.
- For any such consistent formal system, there will always be statements about natural numbers that are true, but that are unprovable within the system.
- The second incompleteness theorem, an extension of the first, shows that the system cannot demonstrate its own consistency.”2
Math collapses as a coherent system under the scrutiny of logic? Is that not a paradox? I thought the presence of a paradox, as 12-step recovery is well known for, was evidence of either illogical statements or false beliefs.
Return to Recovery
Why denigrate either “recovery” or the working a personal 12-step program based on them not being empirically valid? Besides, are there not “other ways of knowing?” And do we not see even math as a system is itself unprovable and incomplete?
The criticism of recovery and of a personal program in the rooms of 12-step recovery on the grounds of math are both in that sense false and, on arrival, in fact – dead – as statements.
A Unified and Inconsistent Model That Works
But rather than study various possible models of recovery, and compare how they compete on mathematical or empirical grounds, can we not turn the lens of observation onto the individual phenomenology of personal recovery?
Doing so would provide (like math itself) a unified and inconsistent model that works, imperfectly accommodating everything that is, including:
- Recovery-oriented harm reduction3
- Serial recovery where use of some substances has ended and use of others has not yet4,5
- Recovery from one substance (like alcohol) while addiction to another (like cigarettes) continues5
- Recovery during medication maintenance6
- Recovery starting even at the peak of severity of illness7
- Abstinence-oriented lifelong 12-step program recovery8
- Recovery continuing after dropping out of support9,10,11
- Being in recovery when you say you’re in recovery
A Final Question
Why criticize individuals and individual differences using incoherent models like math to do so, when our whole system is necessarily inconsistent?
Is it not the case that “one must cultivate one’s own garden?”12,13
References
3Recovery-oriented harm reduction
4White, W., & Kurtz, E. (2006). The Varieties of Recovery Experience. International Journal of Self Help and Self Care. 3(1-2), 21-61.
5Recovery definition – conceptual boundaries
7Jellinek, E.M. (1952). Phases of Alcohol Addiction. Quarterly Journal of Studies on Alcohol. 13(4): 673–684.
8 Narcotics Anonymous (2012). Living Clean: The Journey Continues. Narcotics Anonymous World Services, Inc.
10Disengaged styles of recovery
11Kelly, J. F., Bergman, B., Hoeppner, B. B., Vilsaint, C., & White, W. L. (2017). Prevalence and Pathways of Recovery from Drug and Alcohol Problems in the United States Population: Implications for practice, research, and policy. Drug and Alcohol Dependence, 181, 162–169.
12Condide
13Why Voltaire Said: You Must Cultivate Your Own Garden
Acknowledgment
The author thanks Jason Schwartz for comments on a previous version of this writing.
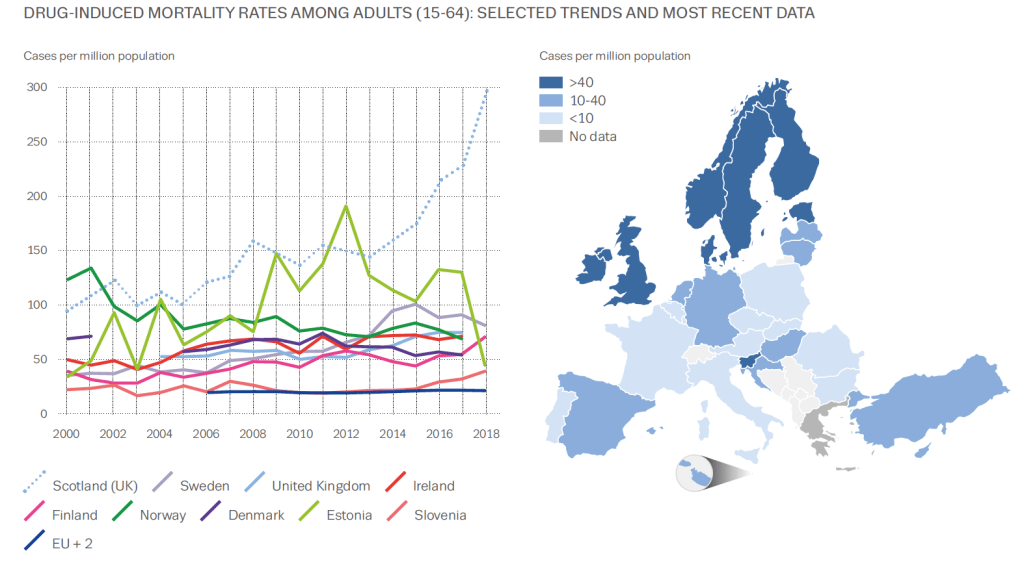 Graphic from European Drug Report 2020: Trends and Developments
Graphic from European Drug Report 2020: Trends and Developments
It’s not often graphs elicit an emotional response, but this one did for me. It’s from the EMCDDA’s recent report on drugs in Europe. The map shows that the UK has high levels of drug-induced mortality compared to most of Europe. But look at the dotted blue line on the graph. That’s Scotland. Worst in Europe and possibly the world.
It’s not a new phenomenon, our high drug-related deaths. The Scottish Drugs Forum makes the point: ‘Drug overdose deaths are preventable. We know how to prevent these deaths and yet they still happen.’
Kindness Compassion and Hope
So what’s being done about it? One of the highest-hit cities is Dundee. A commission set up to look at drug-related deaths took evidence from over 1000 people and made recommendations which included changing the system and culture, having holistic and integrated care and addressing the root causes of drug problems. The report title was Kindness, Compassion and Hope, which feels inspiring.
The Scottish Government has invested in treatment services with a particular emphasis on reaching more at-risk people and retaining them in treatment. Last summer it set up the Drugs Death Task Force, a group chaired by Dr Catriona Mathieson which has highlighted the need for wide distribution of naloxone, an immediate response pathway on non-fatal overdoses, medication assisted treatment (MAT), the targeting of those most at risk, public health surveillance and provision of equity of support for those in the criminal justice system. The Scottish Government has put £1M into research and £4M towards the task force’s six recommendations.
Standards for MAT have been developed, the country has a three week target from referral to treatment, ready access to prescribing, treatment free at the point of delivery, routine overdose prevention training, widespread naloxone distribution, generally accessible injecting equipment provision, low threshold clinics in many places and a high public awareness of the problem. In addition, there is investment in research which looks to find solutions to the problem. But is it enough? – the causes of our drug deaths are complex and rooted in poverty, exclusion, trauma and hopelessness.
A public health emergency
“What we are facing in Scotland is a public health emergency,” Joe Fitzpatrick, Scotland’s Public Health minister stated recently. “I am prepared to consider any course of action that is evidence based to save lives, whether its controversial or unpopular.”
Too controversial for the UK government are drug consumption rooms which Glasgow in particular wants to trial. Drugs policy is not devolved to the Scottish Government and Westminster won’t consider changing the law to allow this to happen, though one crusader is flouting the rules to deliver this currently.
One area in Scotland where consensus is growing is around the likely benefits of shifting to a public health approach. A cross-party parliamentary group, The Scottish Affairs Committee, held an enquiry into the subject and reported at the end of last year. It asked the UK government to declare a public health emergency making the point that the criminal justice approach has failed. It highlighted how current legislation on drugs stands in the way of tackling the issue from a public health slant.
And the UK government’s response? Pete Wishart, the group’s chair described this as ‘the almost wholesale rejection of recommendations.’ The Guardian has suggested this rejection of what multiple experts think is best for Scotland can only fuel calls for independence. When you consider that the UK government hosted a summit in Glasgow last February without consulting the Scottish Government or asking people with lived experience to attend, you begin to grasp the depth of the gulf that separates the two approaches.
The role of visible recovery
I wonder in all of this what the role is for recovering people, recovery communities and the powerful protective effects of developing strong social networks for those most at risk. What if we studied whether developing new social networks had a significant effect on Scottish drug deaths? What if we developed drug consumption rooms which were strongly recovery-orientated with visible recovery present? I suspect, that at the very least, this would boost hope. Hope is often in short supply in addiction, and anything that augments it is welcome.
Perhaps if every outreach service, every injecting equipment outlet and every treatment setting had people with lived experience prioritising the connection of those at most risk not just into treatment but also into a variety of supportive recovery-oriented settings, there could be a positive impact on drug deaths. Perhaps this would help people begin a cultural journey, moving from the culture of addiction to a culture of recovery as Bill White sets out. Not the only thing to be done certainly, our approaches need to be multiple, but something that doesn’t require the permission of the UK Government and which may augment the other interventions.
The Drug Deaths statistics for Scotland for 2019 have been delayed due to COVID, but will be published soon. I’d like to see that dotted blue line on the graph reducing, but that is by no means certain and much remains to be done.
Does mutual aid work? If you are a member of a mutual aid group that you believe is keeping you sober or drug-free, then it’s pretty much assured you will say ‘yes’. That’s understandably not good enough for researchers and some others. Nearly two decades ago, I asked a consultant addiction psychiatrist why he didn’t recommend mutual aid to his patients. ‘There’s not a shred of evidence that it makes a difference’, was his response. It’s a response I still hear fairly frequently. Actually, there was more than a shred of evidence even back then, but it was not at the level of ‘gold standard’ evidence.
Cochrane is a British-based charitable foundation which scrutinises international evidence on health interventions to help stakeholders make informed choices about what is effective and what is not. When Cochrane last looked – in 2006 – at whether there was evidence of efficacy for Alcoholics Anonymous (AA), the findings were disappointing. It wasn’t that there was evidence it didn’t work, but that there really wasn’t much quality evidence about – they could only find 8 studies worth looking at. That review has oft been quoted as ‘proof’ that AA doesn’t work.
All that has changed in Cochrane’s most recent review of the evidence headed up by John F Kelly, Keith Humphreys and Marica Ferri. There are now 27 studies involving over 10,000 people which meet the strict criteria for analysis. The large document capturing the evidence and what it means has just been published.
Kelly, Humphreys and Ferri looked at randomised controlled trials (RCTs), quasi-RCTs and non-randomised studies that compared AA or Twelve-step Facilitation (AA/TSF) with other interventions, such as motivational enhancement therapy (MET) or cognitive behavioural therapy (CBT), variations in TSF, or no treatment at all. (Twelve-step facilitation is designed to increase AA participation). The reviewers also looked at healthcare costs. Those participants in the studies were patients with alcohol use disorder who were there voluntarily.
They wanted to see if AA membership was associated with abstinence, reduced drinking days and reduced healthcare costs. There were some caveats to some of the studies which cover potential selection bias and poorer quality methods, but overall the evidence was sound.
There is a wealth of findings and I recommend reading the review or at least a summary, but I’m going to pick out a couple of the headlines.
AA/TSF when it is manualised (using specific guidance in delivering it) is better than other interventions (including CBT) at helping those with alcohol use disorder reach continuous abstinence. Not just at one year, but at two and three years after the intervention.
AA/TSF when it’s not manualised is as good as other interventions and there is evidence that it saves health care costs compared to other interventions.
That’s pretty impressive.
The authors say:
There is high quality evidence that clinically-delivered TSF interventions designed to increase AA participation usually lead to better outcomes over the subsequent months to years in terms of producing higher rates of continuous abstinence. This effect is achieved largely by fostering increased AA participation beyond the end of the TSF intervention. AA/TSF will probably produce substantial healthcare cost savings while simultaneously improving alcohol abstinence.
So what does it mean for practice? The authors say:
A relatively brief clinical intervention (AA/TSF) can help people with AUD to become engaged in a long-term, freely available, community-based, recovery support resource that can help them sustain ongoing remission. If people with AUD are opposed to attending AA, despite the strong evidence for its potential to aid recovery, clinicians might consider linkage to alternative mutual-help organisations as they may confer benefits at similar levels of engagement.
John Kelly quoted in the New York Times said:
These results demonstrate A.A.’s effectiveness in helping people not only initiate but sustain abstinence and remission over the long term. The fact that A.A. is free and so widely available is also good news. It’s the closest thing in public health we have to a free lunch.
Keith Humphreys said:
For people already in treatment, if they add A.A. to it, their outcomes are superior than those who just get treatment without A.A.
And how does it work? Kelly, quoted in Medscape News said:
The camaraderie inherent in AA and the lived experience of active addiction and recovery can reduce stigma effects — feelings of shame and guilt. The supervision and accountability that an AA sponsor (mentor) can provide has been shown to be very helpful in maintaining sobriety.
“Rigorous studies” have demonstrated AA reduces relapse risk by “helping individuals change their social networks” and “engage in a lifestyle more suited to continuous sobriety.”
It seems the standard and oft-seen negative response as to whether Alcoholics Anonymous works will now need to change, though of course it will only work if addiction professionals and others actively link their clients and patients into AA.

This is a version of a blog I published a few years ago, but thought it still relevant today.
Doug Sellman is a professor of psychiatry and addiction medicine in New Zealand. In 2010 in the journal Addiction, he attempted the difficult task of distilling the ten things you need to know about addiction from the research of the last thirty years. No mean feat.
Well, what are they?
1. Addiction is fundamentally about compulsive behaviour. In normal behaviours, the control in our brains is top down. In addiction the cortex (the decision making bit of the brain) becomes ‘eroded’ to a ‘dehumanised’ compulsion. Sellman outlines the well-studied brain circuits involved, and points out how this view creates one of the defining marks of addiction: continuing to use despite negative consequences.
2. Compulsive drug seeking starts outside conscious thought. The debate about free will (and as the prof says ‘free won’t’) gets complicated here. Apparently the conscious part of our brain is about a half second behind imprinted learned behaviours. The lag and its effects are exaggerated in addiction and well learned patterns including cues call the shots over the ‘higher’ brain’s ability to avoid damaging choices. Result: illogical self-harming behaviours continue.
3. Addiction is about 50% inherited, but it’s much more complicated. Genetic and population studies show a strong genetic element for addiction with some folk being more vulnerable than others. It gets complicated because it’s not just about a single gene or even a few, but possibly hundreds, and even then they interact with infinite variations in environment. This is not about ‘nature versus nurture’, but represents a ‘new interactive model of nature via nurture’.
4. Most people with addictions who come for help have other psychiatric problems as well. For those wanting to move away from the medically dominated model of treatment, this is a big obstacle. 75-90% of those asking for help from services have diagnosable mental health problems including depression, social phobia and post traumatic stress disorder. Alarmingly though, many of our big treatment studies have excluded people suffering from mental health problems. For those of us involved in providing help for those wanting to recover, we will need to ensure that mental health needs are not overlooked. On a personal note though: I do hold a hopefully healthy observation that many of the psychiatric labels we pick up as active addicts melt away in recovery without the need for psychiatric treatment.
5. Addiction is a chronic relapsing disorder in the majority. This was the most challenging of the ten findings for me to simply accept. Prof Sellman says that fewer than 10% of those going through treatment will experience continuous long-term abstinent recovery. He does point out that life will be better for many after treatment and that we need to accept relapse as part of the deal for many. Not doing so will prevent folk coming back for help. There is a tension in this for me between instilling hope and optimism and being unrealistically positive. Other research gives more hope for longer term outcomes suggesting more than half will achieve remission.
[Part 2 is here.]
Event Description
On behalf of the NC Department of Health and Human Services, the Technical Assistance Collaborative will offer a two part web-based training for both LME/MCO and service provider staff on developing a better understanding on how the Section 8 Housing Choice Voucher (HCV) Program is administered by your local Public Housing Authority.
In addition, practitioners will develop a more thorough understanding of the HCV eligibility, application, screening/denials, and waiting list processes.
Finally, practitioners will be offered an overview of how to use a reasonable accommodation request to support a HCV applicant throughout this process.
The training will be offered through two 90 minute webinar sessions that will combine a specialized presentation followed by a question/answer session. This is part two of the training. The 90 minute counterpart to this session will take place on January 20, 2022 from 11-12:30 pm.
Participants are expected to attend both sessions.
Register in advance for this webinar:
https://zoom.us/webinar/register/WN_V_p2J2NGRx6hwNf9KHfNAQ
Event Description
On behalf of the NC Department of Health and Human Services, the Technical Assistance Collaborative will offer a two part web-based training for both LME/MCO and service provider staff on developing a better understanding on how the Section 8 Housing Choice Voucher (HCV) Program is administered by your local Public Housing Authority.
In addition, practitioners will develop a more thorough understanding of the HCV eligibility, application, screening/denials, and waiting list processes.
Finally, practitioners will be offered an overview of how to use a reasonable accommodation request to support a HCV applicant throughout this process.
The training will be offered through two 90 minute webinar sessions that will combine a specialized presentation followed by a question/answer session. This is part one of the training. The 90 minute counterpart to this session will take place on January 27, 2021 from 10-1130 AM.
Participants are expected to attend both sessions.
Register in advance for this webinar:
https://zoom.us/webinar/register/WN_HT--nAwDSnGMsZO4oQ8i9w
After registering, you will receive a confirmation email containing information about joining the webinar.
U.S. Department of Justice Announces FY 2021 Funding For Treatment Courts
NADCP is pleased to announce U.S. Department of Justice grant solicitations to support adult drug courts, juvenile drug treatment courts, tribal healing to wellness courts, DWI courts, and veterans treatment courts have been released.
Bureau of Justice Assistance Adult Drug Court and Veterans Treatment Court Discretionary Grant Program:
Category 1: Implementation grants for veterans treatment courts Award amount: $500,000 each
Award period: 48 months
Category 2: Enhancement grants for operational veterans treatment courts
Award amount: $500,000 each
Award period: 48 months
Category 3: Grants for operational treatment courts or treatment courts “fully ready to implement”
Award amount: $500,000 each
Award period: 48 months
Category 4: Grants for implementing statewide strategies to support treatment courts
Award amount: $1.5 million each
Award period: 48 months
Applicants are required to complete a new two-step submission process:
March 3, 2021: the SF-242 and SF-LLL must be submitted to Grants.gov
March 17, 2021: the full application must be submitted to JustGrants
BJA will conduct an applicant webinar that includes a detailed overview of the application and review of submitted questions. Date, time, and registration details for the event are coming soon.
Office of Juvenile Justice and Delinquency Prevention
Juvenile Drug Treatment Court Program:
Category 1: Planning and implementation grants for juvenile drug treatment courts
Award amount: $600,000 each
Award period: 48 months
Category 2: Enhancement grants for operational juvenile drug treatment courts
Award amount: $750,000 each
Award period: 48 months
Applicants are required to complete a new two-step application process:
February 5, 2021: the SF-242 and SF-LLL must be submitted to Grants.gov
February 19, 2021: the full application must be submitted to JustGrants
OJJDP will conduct an applicant webinar that includes a detailed overview of the application and review of submitted questions, January 12 at 2:00 p.m. ET. Register here.
Additional Information for Applicants New this year, grant applicants must comply with Executive Order 13929 Safe Policing for Safe Communities. See the grant solicitations for details on complying with the order.
For technical assistance with submitting the SF-424 and SF- LLL in Grants.gov, contact the Grants.gov Customer Support Hotline at 800-518-4726 or email at support@grants.gov.
For technical assistance with submitting the full application in DOJ’s Justice Grants System (JustGrants), contact the JustGrants Service Desk at JustGrants.Support@usdoj.gov or at 833-872-5175.
The post BJA and OJJDP grant solicitations now open appeared first on NADCP.org.