
I recently read this article envisioning minimally disruptive treatment for opioid use disorder.
People who use drugs have long called for reforms to make opioid use disorder (OUD) care more patient-centered and less disruptive. Their calls align with broader healthcare transformation efforts, particularly to create “minimally disruptive” systems. Minimally disruptive medicine (MDM) is a “patient-centered and context-sensitive approach” focused on supporting patients’ life goals and health “while imposing the smallest possible treatment burden on patients’ lives.
My first reaction was to reflect on the reality that, over the years, most of my clients needed very significant disruption in their lives to achieve recovery — disruption in their social networks, cognitive models, emotional regulation, sleep, diet, family relationships, etc. Most of that necessary disruption occurred in the context of contact with addiction professionals and other people seeking recovery in treatment and mutual aid settings. That disruption is an essential part of the journey to becoming “better than well.”
I have that reaction as someone who has been a leader in efforts to implement a low-threshold prescribing model in an emergency department. However, I see that low-threshold practices as something akin to first aid and emergency care, rather than an effective treatment for a chronic illness. My wish is that those interventions prevent death, temporarily stabilize patients, and serve as an opportunity to engage the patient in a more comprehensive model of care.
I also recently came across the campaign Program, not a pill. The campaign appears to be a response to growing pressure in recent years to frame medication as an effective treatment on its own.
The majority of people with OUD have more than just OUD, and the medications don’t work for those other issues—common co-occurring conditions include other substance use disorders, mental health problems, difficulty functioning or working in society, social problems, etc. Comprehensive treatment programs can individualize care for each patient based on their own strengths, weaknesses, conditions and circumstances.
Not all 11 symptoms of OUD always respond well to medication treatment, so multiple interventions are necessary for the patient to stop use. That is, even if the physiologic symptoms are rather well addressed with medication, many patients continue to struggle.
Also, just this week, the Wall Street Journal has been reporting on the shortcomings of multiple digital behavioral health providers. Many of these services started with a vision of minimally disruptive care. Their reporting raises questions about whose needs are met with that model — the patient, or the treatment program?
These reactions, in no way, invalidate the Englander article’s critique of maximally disruptive practices. There’s no question that some disruptive practices are rooted in or propped up by stigma. The pandemic has provided a helpful opportunity to step back and examine some of those practices.
Yet, it also feels, to me, like we’re approaching an inflection point in the opioid crisis, where many families, policy-makers, patients, and providers are recognizing that we cannot prescribe our way out of the opioid crisis. This seems particularly important at this moment, as opioid settlement dollars flow into states and localities and, often, the easiest lift is to invest it in medications. (Despite the irony of returning restitution from pharmaceutical companies to pharmaceutical companies.)
So… where do all of these mental meanderings lead me? To be sure, some people will thrive with minimally disruptive models, but many will suffer and die without much more disruptive models. There’s a lot of variation in people’s pathways into addiction, their experience in addiction, and their pathway to recovery.
I suppose, rather than minimally disruptive or maximally disruptive, we ought to be focused on strategically disruptive models of care that do not rely on coercion and instead provide visible, realistic, and comprehensive pathways to recovery that will attract people voluntarily. It sounds easy, but this model was envisioned more than 20 years ago and, despite countless proclamations to the contrary, it’s never been realized at any large scale. It also runs against the zeitgeist (see here, here, and here), which frames patient-centered as organized around the patient’s short-term preferences that are often explored and understood in the context of systems and choices that offer no visible and realistic path to flourishing.
Thank You for an Incredible 2022
This year, we at NADCP are grateful for so much. 2022 saw both a welcome return to normalcy and continued innovation and growth. First and foremost, we want to say thank you. This year, the treatment court field continued to display unparalleled resilience and creativity. As a community, we’ve risen to meet the challenges of our times while ensuring we leave no one behind, especially our most vulnerable community members dealing with substance use and mental health disorders.

Nothing demonstrated our field’s strength better than RISE22, where you absolutely shattered all previous attendance records. In July, 7,700 of you descended on Nashville for an unforgettable conference experience and long-awaited in-person reunion. (And we could not be more grateful for one last hurrah with All Rise Ambassador Leslie Jordan.)
Stay tuned in the new year for all things RISE23!
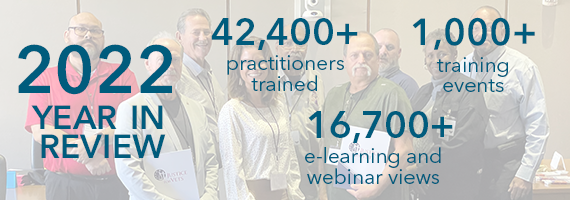
In 2022, we tripled the number of training events and doubled the number of treatment court practitioners trained over 2021! The NADCP E-Learning Center also saw massive growth, more than tripling the number of online courses and webinars viewed and completed. These numbers would not be possible without the support of our federal partners and your constant striving to know and do the absolute best you can for the individuals you serve each day.

Together, we continued to tell powerful stories of the exceptional work treatment courts are doing in communities across the country in the news and on social media. Thanks to you, millions across local, regional, and national media outlets have learned about saved lives, reunited families, and tangible justice reform.
We hope you and yours have a wonderful, safe holiday season.
We cannot wait to continue serving you in the coming year!
The post Thank You for an Incredible 2022 appeared first on NADCP.org.

I’ve been hearing a lot lately about the difficulties in San Francisco related to severe SUDs among people experiencing homelessness. And more pointedly, I’ve been hearing about the death rate by overdose among those living in what I understand to be housing for these people provided by the city.
Simultaneously, I’ve heard reports about leaders in government (local, the state level, etc.) and in the SUD area at the national level, struggling with this puzzle in San Francisco.
Meanwhile, I’ve also had reports come across my view concerning significant financial allocations for broad use of contingency management to help people struggling in these ways, and to help cities improve their responses in these situations. And in that way improve the ecology of their cities.
A number of things come to mind for me in this context. One of them is the question, “What can San Francisco learn from Tehran?”
By that I mean, “What can leaders in the USA gain from partnering with those in other countries who have seemingly found locally relevant solutions, centered in people rather than professions, and are sustainable within existing local resources?”
An example of this kind of success is found in Iran and it’s called Congress 60.
For those not familiar with Congress 60 here are:
Sometimes it helps to learn from outside your discipline (a NIATx principle) and from an entirely different context (so we can see and hear and think in new ways).
The other thing that comes to mind for me is a set of lessons learned about contingency management.
During the lifespan of the Behavioral Health Recovery Management project (BHRM; 1998-2007 or so), we had a number of efforts including clinical dissemination of evidence based practices, best practices, and promising practices. These were per guidelines written for us by the first-author national experts in each area of improvement.
When we implemented contingency management in our outpatient methadone maintenance program (to help raise group attendance) we noticed that those pulling the “JUMBO” prize always returned the winning ticket to the fish bowl that held the tickets. We finally focused-grouped and asked “Why?” We were told very plainly that carrying the large screen TV down the street wasn’t safe.
In those years we partnered with other systems to build and run an FQHC (providing primary care, psychiatric care, SUD services, and access to public entitlements for housing and a whole range of those services). In doing so we were early innovators in embedding primary care and dentistry inside our OP psychiatric buildings. We found the show rate for a free dental cleaning was relatively high, and during that visit we could support with added psychiatric care down the hall.
The lesson learned was this: embed various kinds of services inside a location. People will come for what they want and need, and sometimes you can help by adding in less popular but equally critical assistance. That is to say, getting better initially in the way defined by the individual is contingency management (a relief and a reward). In that way you don’t define the “prize” and wellbeing begets other wellbeing.
In closing, here’s a link to a previous post about NA in Iran. That post includes a link to an audio upload that I find most inspiring. The upload comes to mind for me around the topic of culturally relevant local solutions that are sustainable and emerge from the community.
“I believe that the community – in the fullest sense: a place and all its creatures – is the smallest unit of health and that to speak of the health of an isolated individual is a contradiction in terms.” – Wendell Berry

We need to change how we think of recovery community organizations across our national care system. What is done is far too often managed by agencies not grounded in recovery community or narrowly funded in ways not inclusive of the diverse groups served. This kind of change would require us to explore uncomfortable truths and deep structural stigma within our institutions about addiction and recovery and embrace community as the true healing agent that it is.
We don’t collaborate with recovery community in ways that support its varied resources and strengths. To do so is perhaps the most important thing we could do to augment healing across our entire care system. As a corollary, we know that addiction counseling does not work well when it is overly prescriptive. Care must be individualized and engage the patient in ways that work for them for it to be effective. Why do we fail to apply this very same critical lesson to recovery community level engagement?
I started thinking about this after I ran across a post by Jason Schwartz – Sentences to Ponder. I then ran across the identical referenced section while reading Bill White’s retrospective – Recovery Rising:
“…I do want to suggest that something got lost along the road to professionalization. What got lost was a relationship between two people that transcended the roles of counselor and client. What got lost was our deep involvement in the community and in local communities of recovery. What got lost was our recognition of the power of community to heal and sustain people. John McKnight in his recent book, The Careless Society: Community and Its Counterfeits, argues that compassion shifted from a cultural value to a job description as paid helping roles replaced functions of families, extended families, neighbors, co-workers and friends. He argues that we don’t need more agencies or larger agencies, but that we desperately need more community. In medicalizing alcohol and other drug problems in hopes we could escape its social stigma and moral censure, we turned our backs on the power of community and created an ever-growing distance between ourselves and those we are pledged to serve.”
Bill was writing about Robert McKnight book, Careless Society: Community and its Counterfeits. We do great harm to the community we serve when we prescriptively dictate a narrow set of goals for them. We rob agency from the community and improperly shift power to the external agent. In a parallel process, one of the things that make addiction counseling so special is that when it is done properly, it holds space for healing in a spirit of humility and deep empathy. Bill White describes it well in a piece he did for Counselor Magazine in 2004 titled “the historical essence of addiction counseling.” It honors healing as a highly individualized process not under the rigid control of the counselor.
Honoring Individuals in Care by Holding Space to Explore Their Inherent Strengths and Resiliency
Seasoned clinicians know that we fail the people we serve when we are overbearing or too prescriptive in the therapeutic relationship. Reflecting on my early years as a counselor, I learned fairly quickly that my way was not the best way or even the right way.
Like many new counselors, I made a lot of mistakes. I thought I knew what the person needed to do and could essentially dictate their care. My false expectation was that I would tell them, they would listen, and change would occur. Thankfully, I learned quickly and overcame my misguided thinking. I learned change is a highly individualized process. People must be involved and steer their own recovery process for it to work over the long term.
In those early days, I lacked insight into the full spectrum of strengths the people I was working with possessed. Most of our forms in our service systems focus on deficits when what we should emphasizing is their strengths and the ecology of the communities they live in. People are so very much more than the labels and deficits endlessly delineated in the paperwork we all gathered every time they drew the courage to walk through our doors.
My effectiveness dramatically improved as I learned more of the craft of being a good counselor. I listened more deeply and reflectively. I helped people explore who they were, why they reacted as they did and most importantly the incredible resources they had, but far too often had hidden from themselves. This kind of change takes time and open examination. I was gifted with good mentors and a care system that did not jam people through the process too quickly and fail them in the long run.
I learned so much from the people I was privileged to work with. I learned people are resourceful and resilient. I learned that people who walked into my offices in rags and carrying all their possession on this earth in a trash bag were capable of dramatic change beyond either of our most optimistic initial expectations. I learned that every individual has resources we miss unless we hold safe space for them. A place to explore and nurture the immense capacity for positive change every human possesses. A process that heals people in ways I could never predict or control.
It healed me too. It helped keep me stay vital despite what was occurring around me. The work of helping people within our public care systems is profoundly difficult. I have witnessed a lot of pain and destruction. I have seen and experienced a great deal of trauma. Our systems, insensitively burying us in paperwork, even as we tried to wade through it to help people heal in ever shorter durations of care at lower levels of intensity than what the person needed to get better. I am glad my formative years occurred before services became so constricted.
There is a dark side of our care systems just like every other institution, yet through it all, I, like many other veteran workers who stayed with the work saw that we could, at times be part of a miracle. I have spoken to a lot of service providers and every one of them to a person identified this is why they stayed doing the work, to be small part of the transformative process. To help nurture healing which emerges as hope, purpose and connections are restored.
Honoring Recovery Community as Force of Transformative Healing with Inherent Strengths and Resiliency
I took on a project a few years ago to understand how the New Recovery Advocacy Movement came to be. There would have not been a movement that transformed the way that America understands and talks about recovery without the SAMHSA Recovery Community Support Program (RCSP) grants. Having conducted a number of key interviews with the original grant recipients, the federal grant officer was identified by several interviewees as key to what was accomplished. I interviewed Cathy Nugent to try and find out what it was that she did that helped them come together.
I learned she was a clinician skilled in the art of group process. She brought the grant holders together and helped them see their own strengths. She acknowledged that she was not an expert on recovery, that people in recovery are the real experts. She used her skill set to help those initial RCSP grant holders to develop their inherent strengths.
I once heard Don Coyhis, founder of White Bison, and a key leader in the Wellbriety movement talk about that grant. He shared from a podium about being asked to conduct it using evidence-based practices, He noted that the Native American community had several thousand years of what worked for them and asked how many years of evidence the federal government had.
In an act of wisdom the strengths of this community were respected. They were not diminished by the bureaucracy. Honoring the strengths of that community was the proper action and illustrative of what our system must do more broadly. Communities are diverse. Each has its own culture. They can blossom when provided the proper resources. A sum far greater than its individual parts.
How we fail people in care and communities of recovery when we do not hold space for them:
- We rob them of their own autonomy and stifle their inherent creativity.
- We fail to honor their inherent strengths by restricting them to our limited vision of what they can accomplish.
- We limit their capacity to actualize and help their own members heal in ways that they know far better than we do.
- We impoverish our entire system from a deeper reservoir of resources, skills and social connections to draw from.
What would recovery look like if we supported recovery in communities in ways that honored community diversity and strengths? I imagine what would happen is similar to what happened when I shifted my individual practice, and I was more open to possibility. The people I served went farther than I could imagine when I got out of their way.
What a lesson. What possibility.
We have not done nearly enough to unleash the power of change waiting to emerge from within our recovery communities across America. We stand on the verge of nearly infinite possibility. To deeply honor and support the healing power of community would be to shift our paradigm of healing to the exact thing our nation needs more than anything else at this point in history. More cohesive community.
I dare to imagine we can accomplish so much more than we are now.
I hope you do too.

Yesterday’s post about efforts to support recovery in San Francisco brought some of Bill White’s blog posts and this video from the HBO Addiction series to mind. (The video is showing its age with respect to some of the language and content, but it conveys some very salient lessons that haven’t changed.)
From Bill White:
Physical places and sociocultural contexts exert profound effects on human behavior–a reality too often ignored within biological models of addiction. The repertoire of behaviors that constitutes the states of addiction and addiction recovery are far more than an expression of intrapersonal vulnerabilities and strengths–more than a mirrored expression of genes, character, and personality. Personal behavior can reflect the influence of or domination by the ecosystems in which one is nested/trapped. This suggests the need to extend our focus beyond the intrapersonal to the ecology of recovery–creating social contexts that elicit recovery and suppressing contextual factors that increase risk of addiction.
So, do we continue to send fragile recoveries into environments in which only the strongest recoveries survive? Or do we build recovery-friendly communities in which even the most fragile recoveries have a chance of survival? Those are the questions we face as a country and as people working in the addiction/recovery arenas. We must always attend to recovery at a personal level, but we must also think about recovery in its local, regional, national, and global contexts. Both addiction and recovery are a reflection of the ecologies in which they are nested.
This article from the San Francisco Chronicle caught my attention this week. It illustrates the challenges big cities are facing with the combination of the behavioral health crisis, the aftermath of the pandemic’s disruption, noncarceral responses to drugs, the lack of affordable housing, social responses that frame addiction as secondary to other problems, and the absence of systems of care that deliver addiction care of adequate quality, intensity, duration, and scope.

The article focuses on overdose deaths and the reality that, in recent years, more than 40% of OD deaths in the Tenderloin occurred in sites used to house homeless people, and more than 16% of the city’s OD deaths occurred in single room occupancy setting that are part of the city’s housing program.
“We take people off the streets and put them in this environment they’re not ready for — due to mental illness, or trauma or substance abuse — and sometimes they get worse,” he said.
Even if people like Jackie want to live in supportive housing units where drugs are not tolerated — a model sometimes referred to as recovery housing — there are no permanent, publicly funded options for them in San Francisco. Currently, a formerly homeless person seeking a sober living environment would need to enter a temporary rehabilitative program rather than long-term housing.
So… they don’t have recovery-safe housing and the alternative is treatment. What happens when they complete treatment? Where do they live then?
Cohen said that the agency has heard from some tenants who would “prefer to be in a sober environment and have more choices within” permanent supportive housing. But, Cohen said, HSH’s stance is that abstinence-based programs are “not an evidence-based best practice” and therefore the department has no plans to pursue the model.
This is just not true. There’s considerable evidence supporting recovery housing. It’s not just a few studies and it’s not a recent development.
Sober living environments raise difficult legal and ethical questions, according to some drug policy experts. Critics say residents may hide their drug use at the worst possible time: when their tolerance has worn off and they’re most at risk of overdosing. The model could create a revolving door back to the streets as tenants are kicked out for using.
These concerns represent real challenges to the model, but they are not unsolvable. Systems of care and providers ought to be held responsible for developing and using processes to maintain engagement, restabilize relapsed residents, adjust treatment plans accordingly, and provide a pathway to maintaining or re-entering housing. There also ought to be safety net services for residents who cannot be restabilized and re-engaged. When residents know these processes exist they are more likely to report their relapse or the relapse of a housemate and the addiction can be interrupted–preventing overdoses.
Residents and patients also ought to participate in meaningful informed consent at multiple intervals throughout their early treatment and recovery journey, and they ought to have easy access to the pathway of their choosing with continuous recovery support.
Still, a growing coalition of advocates, including San Francisco Supervisors Ahsha Safaí, Catherine Stefani and Matt Dorsey say the city should explore more types of housing programs that would allow people to live in a drug-free environment.
“We should do more to make sure that people who have substance use disorder have more options than just being in an SRO in the Tenderloin where drugs are surrounding them,” Stefani said in an interview. “It is ridiculous to think that anyone can recover in those circumstances.”
What I appreciate from these advocates is their refusal to turn policy responses into false choices between protecting the lives of people who are using drugs, people choosing treatment/recovery pathways involving agonist medications, and people choosing agonist-free pathways.
One of the other important things I detect in Dorsey’s San Francisco Recovers model is the way they view people with addiction.
Years ago, I was involved in the development of an SUD program for young people in the criminal justice system. A partner in the development of that program said that “we can view these kids as perpetrators, victims, or resources.” Of course, one doesn’t have to cancel out the others, but it was a good reminder to check our mental models and approach those kids as resources.
I sense that same spirit in this model. These aren’t perpetrators to incarcerate or isolate. They aren’t victims to pity, infantilize, and expect nothing from. They are resources that need some help at the moment.
UPDATE: A friend just commented that this is a reminder of how easily compassionate and well-intentioned responses to addiction can devolve into something that resembles an addiction hospice. And, when we construct addiction hospices, we shouldn’t be surprised that people die.
As SMART Recovery meeting facilitator Jeffry Muhleman sees it, the journey to a full-blown substance use disorder is never intentional. “The crazy thing is that when you take your first drink or first hit, nobody tries anything and says, wow, that’s so good I’m going to become addicted to that.”
For Jeffry, it began in 2008 at a New Year’s Eve party where he tried crystal meth for the first time. From there he tumbled down a twelve-year rabbit hole of substance use, bad choices, and legal trouble. Once he found SMART, his journey turned in a whole new direction.
Jeffry attended a variety of meetings and found that some resonated with his experiences more than others. Then he got to thinking, “Being an out gay man, I realized that there was really a need in the recovery community for meetings that are appropriate [for individuals who identify as LGBTQIA+].” Motivated by the value he found in SMART, he decided to become a facilitator and start a meeting specifically for members of the LGBTQIA+ community. But that didn’t mean he wanted to change the way SMART Recovery works.
Jeffry believes that SMART Recovery can work for anyone regardless of sexual orientation or gender identity. That said, he also supports the availability of population-specific meetings. “The reason SMART offers meetings for the LGBTQIA+ community (and other groups) is to provide a forum where common experience and unique understanding inform the conversation.”

Jeffry notes that humans are inherently familial and social, and sharing recovery with those who can closely identify with one’s experience is very beneficial. He also points to the value of therapies that increase a person’s self-awareness and mindfulness, along with the use of SMART tools.
It all comes together in a supportive way for individuals, no matter their perspective or experience. Jeffry says every SMART meeting he’s attended has been safe, and the sheer variety of meetings creates a successful recovery pathway that is available to all.
As seen in Jeffry’s story, when one person decides to help another by giving of their time and energy, it makes a large impact. Jeffry took what he learned from participating in support group meetings and started his own meeting serving the LGBTQIA+ community. His contribution has made it possible for SMART to reach more individuals who are asking for support.
Your year-end financial contribution will be put to work immediately to make additional efforts like this possible. Like Jeffry, you will help more individuals embrace Life Beyond Addiction.
Additional Resources
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to 988 Suicide & Crisis Lifeline @ 988, https://988lifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
The need to save lives and reduce negative health outcomes from drug use is unprecedented. In 2021 alone, the overdose epidemic took the lives of more than 107,000 people in the U.S., according to provisional data from the Centers for Disease Control and Prevention. These deaths were largely driven by fentanyl, sometimes contaminating or taken in conjunction with other drugs. This includes stimulants as well as opioids. There are many other health consequences of addiction, including the transmission of infectious diseases like HIV and hepatitis C.
Enabling people to access treatment for substance use disorders is critical, but first people need to survive long enough to have that choice. Other consequences of drug use, such as infectious disease transmission, must also be mitigated. The United States’ overdose crisis requires bold, evidence-based actions to save more lives, which is why NIH is announcing a $36 million, five-year investment in research to reduce the overdose epidemic and improve care access for people who use drugs through the establishment of a harm reduction research network. The network, funded by the NIH Helping to End Addiction Long-term Initiative (NIH HEAL Initiative) through the National Institute on Drug Abuse, begins this year with nine research grants and one grant to establish a coordinating center.
The projects funded by these grants will test harm reduction interventions so that we can develop evidence-based actions to help prevent overdoses and save lives. Research projects will also assess how well some existing harm reduction programs work, with concrete endpoints like overdose rates. And they will test novel harm reduction approaches meant to gather data on what works, what doesn’t, and acceptability in communities.
Harm reduction is a crucial part of our overall strategy to address the addiction and overdose crises. We know that overdose education and naloxone distribution programs and provision of naloxone to people who take drugs and to first responders saves lives. And, nearly 30 years of evidence shows that access to syringes and other injection equipment helps reduce the spread of diseases like HIV and hepatitis C. People who encounter harm reduction services during active use are often more likely to take steps toward treatment and recovery and stay in better health – saving long-term healthcare dollars and protecting the overall community’s health, too. Other harm reduction techniques such as fentanyl test strips show promise as well, but we need additional data to evaluate their effectiveness and to know more about how to best deploy new tools. The bottom line is that investing in more harm reduction research and tools is key to saving lives.
In addition to overdose prevention, harm reduction programs often have additional benefits, such as linkage to treatment with medications for opioid use disorder (MOUD) as well as other healthcare services provided onsite. Harm reduction programs can be an important way of delivering services to people who otherwise might be afraid of seeking care because of the stigma they encounter in most settings, including traditional treatment settings.
Harm reduction is an important part of reducing the impact of stigma because these services are often staffed by people in recovery or with lived experience of addiction, and thus clients are treated with dignity. This can open doors that lead to treatment, recovery, increased employment, education, and stronger family bonds, as well as reduced drug use.
Several of the studies funded by the new grants will target populations disproportionally affected by drug use and its negative impacts, including Black and Latino/Latina communities, women, and people in rural areas of the country. Multiple projects will examine the efficacy of providing harm reduction services and tools via mobile vans and other on-the-ground outreach.
This is particularly needed in rural areas, where people may need to travel great distances to receive services. Harm reduction techniques must be examined in or adapted to rural settings to see if they can work and are desirable. Overdose deaths involving psychostimulants were higher in rural counties than in urban counties from 2012 through 2020, so some grantees will specifically be investigating harm reduction for people in rural areas who use stimulants.
Projects will also study barriers to accessing harm reduction services more broadly, which can include the physical inaccessibility of services that are located far away from those who need them, and other factors like clinician attitudes that can discourage use.
Some projects are assessing implementation of the evidence-based approach of employing peer counseling and referral, which has been found to increase the ability of programs to reach the hardly reached. All projects will have a community advisory board and/or people with lived experience will have paid positions to support the research. Greater involvement of people with lived experience in all aspects of research is one of the themes of NIDA’s 2022-2026 Strategic Plan.
As is also true of recovery support services, development and implementation of harm reduction over the years has often been driven by peers and people in recovery from substance use disorders—responding nimbly, creatively, and compassionately to the needs of people who are seeking help in their communities. NIDA can help by supporting research that builds on their work, finding out which strategies work, and ways to implement these most effectively for all who need them.
NIH is committed to addressing the overdose crisis with urgency and precision. The number of deaths we are seeing requires us to expand our thinking with evidence-based, scientific action that can meaningfully save more lives. These grants will help us achieve that mission.
For more information about the new harm reduction research network, read the NIH press release. NIH is not providing funds for the purchase of pipes, syringes or needles.
Brian Coon posted a reaction to the NIAAA definition yesterday. I also recently watched the NIH webinar on the definition.
“Recovery is a process through which an individual pursues both remission from AUD and cessation from heavy drinking. Recovery can also be considered an outcome such that an individual may be considered ‘recovered’ if both remission from AUD and cessation from heavy drinking are achieved and maintained over time. For those experiencing alcohol-related functional impairment and other adverse consequences, recovery is often marked by the fulfillment of basic needs, enhancements in social support and spirituality, and improvements in physical and mental health, quality of life, and other dimensions of well-being. Continued improvement in these domains may, in turn, promote sustained recovery.”

I like several elements, including ones that Brian noted:
- It frames recovery as a process and an outcome. (Other recent definitions frame recovery only as a process.)
- It provides clear criteria.
- The criteria address alcohol use.
- It looks beyond drink counting and references improvements in global health and quality of life. (Note, though, that these improvements are not required.)
All that said, it leaves me wanting something different.
As I sat with that dissonance, I decided that it is a fine definition of recovery for Alcohol Use Disorder (AUD) but I find myself troubled by the application of the concept of “recovery” to AUD.
In the webinar, John Kelly discusses (15:30) the challenge of trying to turn a cultural concept (recovery) into a scientific concept. The cultural concept of recovery is more than the reduction (or even elimination) of symptoms and focuses on an additive experience. I think it’s also fair to say that, in the cultural realm, recovery has been more than a process or outcome–it’s been an identity.
Why would something recovering from an illness become integrated into one’s identity? Because the experience of alcohol and other drug addiction is often life-threatening, traumatic, treatment can provide few guarantees, and it often erodes one’s identity. It also transforms an experience of stigma into an identity the individual feels pride in.
So, when you’re talking about recovery as a kind of identity, “recovery from what?” becomes a salient question.
People who faced and survived a life-threatening illness like lung cancer may integrate being a cancer survivor into their identity. The same might be true for groups of people who survive certain disasters. Importantly, those identities may serve as a source of connection to others who share the identity and can be powerful enough as a social adhesive that entire communities are built around them.
This definition puts the following people into the same category of “recovery” from AUD:
- While in college, Henry drank several days a week, spending most of the weekend drinking with friends. During his sophomore year, it was common for him to have as many as 8 drinks on weekend days, but that progressed to 12 during his junior year to achieve the same effect. It was common for him to be hungover on Saturday and Sunday mornings and spend half the day recovering. His drinking caused considerable tension with his parents who believed his drinking adversely affected his grades and his relationships with his family. This was true, but Henry said he wasn’t concerned. After a few rough semesters, Henry decided to cut back to a couple of drinks on Thursdays and 4 drinks on Fridays, Saturdays, and Sundays.
- Shayna started drinking in her teens and drank heavily on weekends, often drinking to the point of passing out. On a couple of occasions, friends needed to take her to the hospital for alcohol poisoning. She tried to cut back, but found herself unable to moderate with any consistency. Shayna got into a good college, but her drinking led to her being expelled due to poor grades. Several relationships ended because of her excessive drinking and her behavior when she was intoxicated. She lost jobs due to her drinking and tried to stop but was unable to, despite her best efforts. Her parents took physical custody of her children because her drinking made her an unreliable caregiver. She entered treatment several times but dropped out or never stopped drinking despite anti-craving medication. She spent time in jail due to multiple impaired driving convictions. She entered treatment for the 8th time, moved into a recovery home for 12 months, got deeply involved in a mutual aid group, stopped going to old hangouts, and developed a new social network of people in abstinent recovery. She struggled with severe cravings to drink, fortunately, these faded slowly as she did the hard work of rebuilding her life.
- Mark had a pattern of alcohol use very much like Shayna’s but also used cocaine, cannabis, and opioids. After a drunk driving accident, Mark found that using benzos helped him reduce his drinking to a few drinks a few times a week. Others have noticed that his cocaine use accelerated following the reductions in his drinking. His drug use is causing considerable functional impairment and he meets all criteria for substance use disorder.
Does it make sense to put these three people in the same category? They’re all in remission from AUD and have ceased heavy drinking.
Would Henry or Mark be likely to identify as in recovery? Might they begin to use that label if researchers, treatment providers, and advocates tell them they are in recovery? Would their loved ones think of them as in recovery? Would it make sense to an observer if we describe them as being in similar states of recovery?
To me, remission seems like a more appropriate characterization of Henry’s experience.
On the other hand, it would seem strange to characterize Mark as in recovery from AUD when he is in the throes of drug addiction.
Would Mark, Henry, and Shayna see themselves as having a shared experience or identity? Would their experiences be helpful or validating to each other? How meaningful is a category that includes such diversity in pathology and problem resolution?
Putting the three of them in the same category may make sense from the perspective of a researcher (I’m not sure that’s true.), but does it make sense from a cultural perspective? Does it make sense to develop research definitions that create discord with cultural understandings (even if their boundaries are poorly defined)? Where there is discord, how do research and cultural understandings interact and influence each other?
The NIAAA (National Institute on Alcohol Abuse and Alcoholism) recently published a definition of recovery.
Here’s the recovery definition from that paper:
Recovery is a process through which an individual pursues both remission from AUD and cessation from heavy drinking. Recovery can also be considered an outcome such that an individual may be considered ‘recovered’ if both remission from AUD and cessation from heavy drinking are achieved and maintained over time. For those experiencing alcohol-related functional impairment and other adverse consequences, recovery is often marked by the fulfillment of basic needs, enhancements in social support and spirituality, and improvements in physical and mental health, quality of life, and other dimensions of well-being. Continuous improvement in these domains may, in turn, promote sustained recovery.
Hagman, B., & Falk, D., Litten, R. & Koob, G. (2022). Defining Recovery From Alcohol Use Disorder: Development of an NIAAA Research Definition. American Journal of Psychiatry. 179. 10.1176/appi.ajp.21090963.
In my opinion the paper is important for our field. Why do I think it’s important? Well, it’s:
- a more recent definition
- from a major academic/research body with national and international weight
- the kind of definition that is rooted in measurement and lends itself to scientific use
- not a recovery definition that is rooted in mere ideas and expressed in ways that are not measurable
The NIH released a videocast discussing the definition. If you click that link and scroll down, you’ll easily find it.
Overall I find the NIAAA definition of recovery remarkable because it states:
- recovery is a process
- recovery is also an outcome
- people can be considered “recovered”
- spirituality is included in the list of things that might improve
- physical health, mental health, and various dimensions of well-being are included
- continuous improvements may in turn help stabilize recovery
- both heavy drinking and its harms are outside of recovery
From a perspective more particular to my exact thinking, this new recovery definition from NIAAA…
1. fail to study drop outs, no-shows, and those that pass away;
2. fail to have long-term care structures for routine maintenance checks, and
3. are usually trained in siloed specialty work and not a wholistic model as well.
Plus, it:
In closing, I’ll say that when I read the definition I liked it right away for a lot of reasons. And one of the main reasons is that to me (as a working clinician with an academic/research bent) it seemed to hold common sense, practical clinical reality and value, and help with measuring. And another main reason is because it seems to hold space for
And something like that seems tight enough and yet messy enough that it might actually help us move forward.
What do you think?