
Experts Answer Your Questions on Evaluating Your Treatment Court
Schedule your one-on-one video conference October 14 or 15
NADCP’s National Drug Court Institute Drug Court U is hosting office hours with our partners at the National Drug Court Resource Center. Get one-on-one appointments with evaluation experts Kristen DeVall, Ph.D. and Christina Lanier, Ph.D. to ask your questions about determining outcomes in your program. Appointments are available Wednesday, October 14 and Thursday, October 15.
Understanding your program’s effectiveness is important to the health and well-being of your participants. Drs. DeVall and Lanier can answer your questions about evaluability assessments, needs assessments, as well as process and outcome evaluations.
Whether your program is new to evaluating outcomes or has been doing it for years, our experts can help you!
Reserve your appointment now! Times are limited.
Just like office hours in college, Drug Court U offers treatment court practitioners the opportunity to schedule one-on-one discussion time with experts and receive individualized, confidential instruction via video chat or conference call.
About Dr. DeVall
Kristen E. DeVall received her Ph.D. in sociology from Western Michigan University in 2008. She is the co-director of the National Drug Court Resource Center and a professor of sociology and
criminology at the University of North Carolina Wilmington. She has conducted evaluations of numerous treatment court programs and other criminal justice initiatives in Michigan and North Carolina since 2004. She has conducted several statewide evaluations, which involved the collection and analysis of both quantitative and qualitative data. In addition, she worked as a case manager for a community corrections program in Michigan for seven years. Overall, her work seeks to bridge the gap between academia and practitioners, as well as influence the development of evidence-based policies and practices.
About Dr. Lanier
Christina Lanier is the co-director of the National Drug Court Resource Center and a professor of sociology and criminology at the University of North Carolina Wilmington. She received her Ph.D. in sociology from the University of Delaware in 2006. She has extensive experience in the area of grant writing and program evaluation. She conducts program evaluations for specialty courts in North Carolina and is a co-evaluator for a local reentry program. Other recent projects include statewide evaluations in Michigan and North Carolina. Dr. Lanier’s focus is on linking the work of researchers with practitioners to make policy and social change.
The post Experts Answer Your Questions on Evaluating Your Treatment Court appeared first on NADCP.org.
FREE Foundational Training for Adult Drug Courts, Tribal Healing to Wellness Courts, and Veterans Treatment Courts
Application deadline: November 6, 2020
NADCP is pleased to announce that registration for 2021 DCPI Foundational Training Programs is now open for adult, tribal healing to wellness, and veterans treatment courts. All 2021 trainings will be conducted virtually.
The DCPI Foundational Training Programs are for courts that are:
- Pre-implementation
Adult drug court, tribal healing to wellness court, or veterans treatment court still in the planning stages - Post-implementation
Recently implemented programs that have not participated in formal training - In Need of a Refresh
Established programs that have experienced significant turnover in staff - Never Formally Trained and Facing Challenges
Established programs that have never participated in formal training
Benefits of Foundational Training Programs:
- It is a free training program
- 90% of communities that attend this training launch a program
- Operational courts have rated this the best foundational training, whether they were addressing transition or recently implemented
- Our staff and a cadre of nationally renowned treatment court experts and practitioners work with selected teams to implement evidence-based practices, develop policy and procedure manuals, and build team unity
- At the conclusion of the training program, you will have your blueprint for implementation or transition
NADCP’s Foundational Training Programs fill up quickly, and the waitlist is always long. Do not hesitate; submit your application today!
Sponsored by the Bureau of Justice Assistance within the Office of Justice Programs at the U.S. Department of Justice.
The post FREE Foundational Training appeared first on NADCP.org.
4 Reasons Why Acceptance is Essential to Your Recovery

“When I stopped living in the problem and began living in the answer, the problem went away. From that moment on, I have not had a single compulsion to drink. And acceptance is the answer to all my problems today. When I am disturbed, it is because I find some person, place, thing or situation – some fact of my life – unacceptable to me. I can find no serenity until I accept that person, place, thing or situation as being exactly the way it is supposed to be at this moment. Nothing, absolutely nothing, happens in God’s world by mistake. Until I could accept my alcoholism, I could not stay sober; unless I accept life completely on life’s terms, I cannot be happy. I need to concentrate not so much on what needs to be changed in the world as on what needs to be changed in me and my attitudes.” Alcoholics Anonymous (Big Book), 4th Edition, P. 417
The dictionary defines acceptance as the act of taking or receiving something offered–favorable reception; the act of assenting or believing: acceptance of a theory. The fact or state of being accepted or acceptable. You know what acceptance is, you can think through acceptance, but how can one really begin to practice acceptance in a way that supports their recovery?
Understand the importance of acceptance
Acceptance is necessary for your healing process. To practice acceptance, you must acknowledge all of the uncomfortable parts of yourself: your emotions, your thoughts, and your past.
Practicing acceptance is kind of like taking care of the dirty clothes hamper in your room. Throughout the weeks, you fill it with your clothes and it piles up. Work is tiring, cleaning the rest of the house is enough of a chore, and life keeps getting in the way. You know that the hamper is there, but you’ve been ignoring the real mess of clothes inside.
After enough time passes, you may even forget that you own some of the clothes at the bottom of that basket. Finally, the day comes when you acknowledge that the corner of your room is a real mess, you’re short on clothes, and it’s time to do laundry. As you take out each piece to wash them and hang them, you’re acknowledging the separate pieces of the mess, and accepting the situation and the tasks necessary to clean up—much like when you take your personal inventory and accept that you are imperfect, that there are parts of yourself and your psyche that you must work to heal.
Recognize the gifts of acceptance
As you grow and practice acceptance towards yourself, you’re able to be more accepting of others. When we make peace with the fact that everything is exactly the way it is supposed to be in the present moment, you can make peace with the variables of life around you, including other people. Compassion gives you the ability to grow in your own regard, while you also aid in other’s personal journey to self-acceptance.
Embrace the freedom of acceptance
Acceptance—though not an effortless task—is a freeing habit. Anxiety, stress, and depression can often be caused by the unwillingness to make peace with the terms of life. It is human nature to think that one can control and manipulate all of the components of reality, but you simply cannot. Peace and true serenity can only be found once you accept life on life’s terms.
As you find yourself troubled, upset by day to day struggles, situations, and others, remind yourself of the component of the serenity prayer in which you ask for the courage to change. When you’re feeling dissatisfied in those moments, figure out what you can change about yourself to accept the situations and people as they are in that exact moment.
After acceptance, comes gratitude
It’s important to remember that acceptance is not synonymous with tolerance. Acceptance is not the reluctant sigh at the end of a stressful day, nor the disgruntled statement, “it is what it is,” or “this is just who I am,” No, acceptance is total mindfulness grounded in reality.
Acceptance is the realization that your suffering, your anxieties, and stressors, are exacerbated in the moments in which you believe that you can successfully live your life or handle your recovery on your own terms. As you learn to accept and make peace with the way things are in this very moment, you step out of your own way and step forward on the path to growth.
The more often you practice acceptance, the more you will see that each moment has a purpose, a lesson to teach you, a reason for unfolding the way that it does. As you stay present in those moments and genuinely accept them, you may work to find ways to be grateful for life on life’s terms, further strengthening your recovery and improving your quality of day to day life.
***
For more information, resources, and encouragement, ‘like’ the Fellowship Hall Facebook page and follow us on Instagram at @FellowshipHallNC.
About Fellowship Hall
Fellowship Hall is a 99-bed, private, not-for-profit alcohol and drug treatment center located on 120 tranquil acres in Greensboro, N.C. We provide treatment and evidence-based programs built upon the Twelve-Step model of recovery. We have been accredited by The Joint Commission since 1974 as a specialty hospital and are a member of the National Association of Addiction Treatment Providers. We are committed to providing exceptional, compassionate care to every individual we serve.

“Life is pain…anyone who tells you differently is selling something”
William Goldman, The Princess Bride
Pain and addiction are intertwined. Prescribed medication for pain can be a route into addiction. In practice I regularly see people on multiple medications for pain, making treatment of their addiction challenging.
Last year Public Health England found that one in four people were taking ‘addictive’ prescription medicines. It looks like this is eclipsed by the situation in the US with a 2016 SAMHSA report stating ‘an estimated 119.0 million Americans aged 12 or older used prescription psychotherapeutic drugs in the past year, representing 44.5 percent of the population’. A third of this was pain medication.
This suggests there’s a lot of pain around. But pain needs to be addressed appropriately so it’s no surprise that there’s a lot of analgesic prescribing. It’s needed – right?
Well not so fast. The evidence for the benefit of opioids, for example, in chronic pain is pretty dire. Where studies have been done, the follow-up period is generally ultra-short.
So how confident can we actually be that opioids are both effective and safe in chronic pain? Well we can look to the highest standard of evidence, randomised controlled trials (RCTs).
See this flow chart for an analysis of the evidence base to 2012. It’s not particularly impressive to put it mildly. Yet millions of people have ended up on long-term opioid pain medication.
Now the UK National Institute for Health and Care guidance (NICE) has issued draft guidelines for the management of chronic pain. NICE aim to improve outcomes by setting out evidence-based guidelines. What do they say? Well, it’s pretty clear, not to mention stark:
Do not offer any of the following, by any route, to people aged 16 years and over to manage chronic primary pain:
- opioids
- non-steroidal anti-inflammatory drugs
- benzodiazepines
- anti-epileptic drugs including gabapentinoids, unless gabapentinoids are offered as part of a clinical trial for complex regional pain syndrome
- local anaesthetics, by any route, unless as part of a clinical trial for complex regional pain syndrome
- local anaesthetic/corticosteroid combinations
- paracetamol
- ketamine
- corticosteroids
- antipsychotics
This is a pretty revolutionary development and has set the cat somewhat amongst the pigeons. It’s still in draft, so may be modified, but by any measure it’s quite a change.
Reporting on the response to this of the Faculty of Pain Medicine of the Royal College of Anaesthetists who had concerns about category definitions of pain, the Pharmaceutical Journal said that the terminology was “highly confusing and damaging” and that there was a “serious risk” that the recommendations would be taken to apply to all chronic pain. It said that this “essentially” resulted in the guidance “not being fit for purpose”.
GPs have also expressed concerns around limited options with Pulse magazine reporting: ‘NICE has also missed the glaringly obvious contributing factor of social deprivation… chronic pain is almost overwhelmingly a problem of deprivation and despair.’
Given the number of people who present in primary care with chronic pain, I can understand those concerns. Although antidepressants are recommended in the guidance, alternative approaches to prescriptions take time and expertise to deliver. But what does this mean for all those people already on long term medication?
I am left wondering how we ended up with so many people on medication for pain with so little evidence of efficacy. My thoughts turn to Big Pharma and a commentary by Des Spence I read a few years ago in the British Medical Journal (restricted access):
“Research always reports underdiagnosis and undertreatment, never the opposite. Control all data and make the study duration short. Use the media, plant news stories, and bankroll patient support groups. Pay your specialists large advisory fees. Lobby government. Get your pharma sponsored specialists to advise the government. So now the world view is dominated by a tiny group of specialists with vested interests. Use celebrity endorsements to sprinkle on the marketing magic of emotion. Expand the market by promoting online questionnaires that loosen the diagnostic criteria further. Make the illegitimate legitimate”
Is he right?
I’ve been listening to a BBC podcast on my way to work this last couple of weeks which I’ve really enjoyed. Called Hooked, it’s about ‘all things addiction and recovery’ and is frank, funny, well-informed, upsetting, entertaining, resonant, authentic and powerful.
Melissa and Jade share their lived experience but also interview experts and others who are in recovery on a variety of topics including: rehab; relationships; relapse; codependency, porn and sex addiction; mental health; food; sober Christmas etc.
The presenters debunk myths, dissolve shame, educate and reduce stigma in with their unique blend of humour, curiosity and discussion. I recommend it.
It’s available for UK listeners from the BBC website, on the BBC Sounds app, and for people living elsewhere on Apple Podcasts.
Who are you?
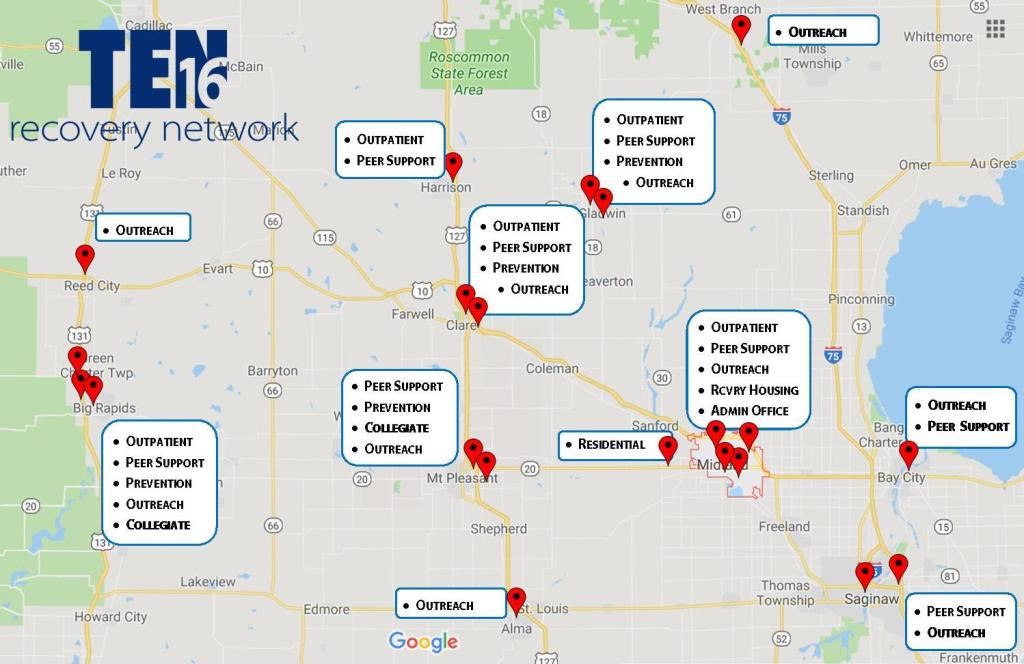
My name is Sam Price, I am the President/CEO for the Ten16 Recovery Network.
Tell me a little bit about Ten16 and your role there.

Alright, Ten16 is celebrating its 40th anniversary this year. I have been here since 2003, so about 17 of that has been on my watch. It started out as a halfway house by the local churches, way back in the day, and that migrated into residential treatment, and then we got into outpatient, and then we got into prevention and then we got into expansion. We started in Midland, Michigan. We are now in 10 different counties; providing outreach in emergency departments, we have residential, recovery housing, prevention, outpatient, drop-in centers, collegiate recovery on three campuses, prevention in four, five communities. So we try and have the full continuum, both vertically and horizontally, to work with folks.
How would you describe the communities you’re working in?
It’s a mixture of mostly rural. Midland is probably more of a suburban community. We started to work in Saginaw, which is more urban. So, it’s kind of a broad mixture, but I’d say mostly tilting towards suburban and rural.
Tell us about your professional experience in addiction and recovery, did you have any SUD experience prior to Ten16?
No, I didn’t. When I was selected to come to Ten16, my wife and I lived in Charlotte, Michigan. She was a teacher for the hearing impaired in Lansing, and I worked at a juvenile justice facility called Starr Commonwealth based in Albion, Michigan. Starr had about 200 residential beds for children that were in the juvenile justice system and had sites really across Michigan, in Ohio, with other community-based programs as well as other residential programs. I’ve always been in the helping field in one fashion or another but hadn’t been in SUD specifically. Midland was our hometown, and we wanted to get home. My wife’s mother was sick at the time. The opportunity came up to come to Midland at Ten16 and they invited me to work there, but it was really my first foray into SUD.
What are you most proud of in your professional life?
I saw that question before, and it really made me think…
I think probably the growth of the organization in these recent years, which has been pretty substantial. I think what has most made me proud is the fact that the staff have this willingness to join me to be bold and pioneer. For example, the thing that’s driving us right now is really kind of two ends of the spectrum in terms of how we view what we’re trying to bring to the community. In the one sense, we know that only 10% of the folks that struggle (with SUD) will walk through our doors or your doors on their own. So, we have intentionally said, “How do we put ourselves in places to get in front of the missing 90%?” And how do we engage them in conversations that may spark the beginning of recovery? That shift has attracted to us a lot of people who want to join us in the pursuit of that real… almost… raw recovery evangelism, if you will. So, in the last five to six years, we have ended up going from one hospital Emergency Department to ten; where we can sit with patients who are in the ED, maybe not even because of their SUD history. Maybe they’re there for a broken arm.
Here’s a great example of who we have a chance to talk with – there’s a time that my wife and I were in the emergency room for our own medical situation as a family. In the curtain right next door to where we were, [because that’s the only privacy that you have in the ED], there was a 72-year-old guy who was in there for some cardiac issues. He was waiting for the cardiologist to come, and the nurse came in to do the health history with him. As she’s talking with them, she finds out that he has been a widower for the last three years. He lives outside of Weidman, which is a town that has a population of maybe 1,000 at best. He’s not living even in the town itself, his kids to live out of the state. And, it’s just he and a cat and a six-pack every night.
Now he’s in the ED for heart issues. That’s what our advocates have an opportunity to do. The nurse can then turn to our staff and say, “Hey, I think you need to talk with this guy.” To us, we think there might be something about the six-pack a night that may be contributing to both his physical heart issues and his spiritual heart issues. We’re able to start that conversation that we never get if we just waited for him to walk through our door it. It’s easy to work with the person who shows up under the influence, or who shows up in the ED med seeking and stuff like that. We have so many rich opportunities to talk with other people who we would never normally be able to talk with and engage them in that change process.
On the flip side, we also know that we have to walk alongside somebody for five years before they can get that remission rate down to a truly sustainable level. How do we change our way of doing business and our way of offering services to folks that would cultivate that? We have totally re-engineered our outpatient practice so that it’s full drop-in. Any time you need to stop in and talk with somebody, you don’t have to have a scheduled appointment. You can stop in. The energy that brings to the staff, because we can have this community approach, has been incredible.
Ten16 is a place to start that journey. They can come to this rich, robust community, which then can introduce them to the natural (recovery) community that exists out beyond our professional walls. So, I think that direction, the energy, and the enthusiasm that the staff has brought to that movement would probably be what I would say is my proudest moment at Ten16.
What keeps you working in addiction and recovery?
It’s funny, people ask me that every now and then. When I was much, much younger, I had an opportunity to experience redemption on a personal level, because I was becoming a person that I didn’t think I was up here [pointing to his head – my self-perceptions weren’t in alignment with my actions]. When I really stepped back and saw where my life was heading, that’s not what I wanted to be. There was a spiritual awakening, if you will, that allowed me to experience this sense of redemption. The richness that that has brought (to my life) since then, is something that I want anyone who is lost and hurt and broken to have an opportunity to find. People that struggle with SUD need folks to help stand in the gap and say, “Hope is here and will be here and we’ll be here as long as you need… until maybe you can experience the same thing that I’ve experienced.”
How has the pandemic affected your work at Ten16?
Well, it certainly has put a cramp on community. We have to be uber-cautious for the safety of the staff and the safety of all the clients. There is a fair amount of concern that comes with that, which has a lot of really unhealthy consequences, particularly for the folks that we work with, because it breeds isolation. Isolation strips away the community that had been holding me (speaking as if a person in early recovery) together, and giving me that encouragement that I’ve been looking for in order to be able to keep moving forward every day.
A lot of that’s been stripped away… Yeah, I (speaking as if a person in early recovery) can get it through a virtual meeting, but that’s not the same as being face-to-face with other folks. So, the loss of that is hard. So, a lot of the coping mechanisms that I had have been stripped away from me, and haven’t been replaced in the same kind of meaningful way, and all new kinds of stressors are kinda coming along for us. So, Ten16 has seen an uptick in relapses. We’ve seen a huge uptick in the hospitals for alcohol-related events. They’ve (the hospital staff) seen a big uptick in methamphetamine and opiate relapses too.
So, as so many others in the press have said, it has a secondary impact when you roll into a pandemic with an (opiate) epidemic. It’s just not a good combination at all. The other thing is that, at the same time that it’s impacting all the folks that we serve, it’s impacting everyone that works here at the same time. It is not like there’s this separation. So, I’m trying to be present for the people who are coming to my care, and I still have to think about my wife and my kids–are they safe? and my extended family and my parents, are they safe? –none of us can escape that. It’s not just impacting the folks that we serve, it impacts all of us. So, it’s hard to turn that noise off, to be present, to help those that are looking to us for care at this time.
What, if any, long-term effects do you anticipate from the pandemic for the field?
It’s hard to know fully, because we’re still so early into it. I’m seriously afraid that it could be another 12 or 18 months that this is going to linger, if we have another wave that comes through. What I don’t know is what that’s going mean to treatment facilities. I’ve already heard that several dozen across the state have already closed, and another several dozen are teetering on the brink of closure.
Because of leaders trying to be safe in the way that they run their programs, there is limited access to treatment beds for those people that need a higher intensity of care. So, access is just going to continue to get crippled, which means getting in for timely service is going to be really, really problematic for folks. There are no easy answers to know how to fix that.
Even when you think of what happens out in the natural 12-step community, and the larger recovery community, even that has been impacted. Can there still be meetings indoors? Even so, you can’t have meetings of more than 10 people. Are there in places in our communities (like churches or community centers) that are even allowing 12-step meetings to be hosted because of some of the risks? So, there are so many ripple effects… I think we’re still just at the tip of the iceberg that we just don’t even know yet.
Again, that’s part of the problem, there’s so much uncertainty and ambiguity that is difficult for people to know how to navigate. There’s no end in sight to that, which gets back into that resilience depletion, right?
Have you seen any benefits or new opportunities in the pandemic?
Certainly the one that everyone turns to is the advent of telehealth, both for treatment services as well as recovery support, peer support opportunities. Again, it’s a blessing and a curse thing. Certainly, it fills in some of that access gap that [with a tool] we never had. Because we are forced to do it has made both parties–both providers and participants–more open to that. We find that, “Hey, this is can be a nice thing for me to be able to have my session, but I don’t have to worry about the headaches of transportation, because I don’t have a driver’s license, or I don’t have money for the bus or something along that line.” So, there are huge wins to that. I can go into rooms and I can find a meeting anywhere across the country. Those are wonderful things. There are limits to those things too, so there’s always the concern that when the pendulum swings or when the policy makes you say, “Oh, look at that.” All of a sudden it becomes a substitution for real community, because we’ve been able to develop this virtual community.
As it continues on, I think it will force us to continue to figure out how we can be more creative–how does it force us out of our boxes? For example, the regulations behind telehealth before were just Neanderthal. No one did it because the regs were so tight. Well, this kind of forced that change, and now that that horse is out of the barn, some of the people that hold the dollars have realized, “Okay, maybe we were a little bit too rigid, too cautious in some of the stipulations that were put into place.” Hopefully, that will allow for more creativity and more freedom, more flexibility to spark innovation.
I think we’re still trying to figure it out and figure out what the rules are, of how you can advance things safely within this… if we have to limit the number of people that are in a room, if we have to wear masks, if we have to be 6 feet apart….there are just so many new factors that we have to sort through, that I don’t think we know fully yet. It forces us to get out of our little cookie-cutter approaches that we’ve been so comfortable with–that has defined how we provide care–so I’m excited to see where it may lead us. All of a sudden we could have opportunities where, yes, we’re here in Midland, but all of a sudden maybe because of telehealth, we’re providing treatment and care and support to people in Ohio, or Wisconsin, or Seattle.
I think [peer support among providers via video conferencing] could be another good silver lining. We have gotten very comfortable doing this kind of stuff and feeling good with it.
We’re just talking about that mid-state meeting… if we could just have an open Zoom meeting for any provider that just wants to talk about the stresses, and the strains, and the struggles of doing virtual care, and all this sort of stuff, why wouldn’t we? Why couldn’t we? Maybe it’s breaking down some of those walls that have held us back.
If you were able to devote yourself to a fantasy project to improve treatment and recovery support, what would it be?
Sam: I think we still haven’t figured out as a system of care of how we go beyond maybe that first year of support. As people grow and mature in their recovery, those recovery needs change–how do we walk alongside them in meaningful, productive, and constructive ways?
We often talk within our organization–how do we help people move from recovery into wellness? As I’m getting some of these early recovery skills down, and I’ve figured out this part… but then there’s the next layer of my relationships or I’m getting my relationship with drugs in that right and healthy and place, but now it’s about, how do I find a career that brings me a feeling of meaning and purpose? Or, how do I get my relationships where that brings me meaning and purpose? How do I keep building upon that, in a way that I have constructed this robust life that we all kind of long for and dream for?
I’ve also seen some of those organizations that have micro-enterprises where they employ their own, and then those employees become the managers of different places, and some of those types of organic businesses or organic opportunities would be so cool to see develop.
Another odd little fantasy that I’ve had every now and then is, “I wonder what it would be like to have an assisted living facility for people in long-term recovery?”
I don’t know why, but [the idea has] always been one of those, “Huh, I wonder… as we age… would that be something?”
I don’t know why, but it’s always intrigued me about that kind of a community, and how would that look differently as we age, when typically medications are being poured on to us, and we’re losing a lot of our normal community… because my friends passed away, my spouse passes away, my kids move away. And, what do we do best as recovering people? Community.
What are the needs of somebody who’s had a long-term history or struggle with addiction? Maybe they have special medical complications that are kinda unique to that niche group of folks.
So again, it’s one of those things that I never spent a lot of time looking into it, but I’ve always been kinda fascinated about it. We’re all getting older!
Event Description
Please register for COVID-19 Provider Call - Oct 1, 2020 3:00 PM EDT at: https://attendee.gotowebinar.com/register/5218202330861960460
After registering, you will receive a confirmation email containing information about joining the webinar.
Closed Captioning: https://www.captionedtext.com/client/event.aspx?EventID=4582433&Customer...
During this call, panelists will present policy updates from DMHDDSAS and DHB representatives followed by an open Q&A session. In addition to DMHDDSAS and DHB subject matter experts we will also have a representative from DHSR on the call to answer questions you might have. In consideration of the limited time we have on the call, we ask that you review the guidance links (below) on the DHHS website and FAQs on the NC Medicaid site to see if an answer to your question has already been provided. These calls will be held monthly on the first Thursday of each month.
As things continue to change and move quickly during the COVID-19 pandemic, please continue to stay abreast of emerging issues, guidance, and policies by visiting:
Broad information and updates: https://www.ncdhhs.gov/divisions/public-health/coronavirus-disease-2019-covid-19-response-north-carolina
Policy and Guidance updates: https://www.ncdhhs.gov/covid-19-guidance
COVID19 Executive Orders: https://www.ncdhhs.gov/divisions/public-health/covid19/executive-orders
Thank you for your dedication and service to North Carolina BH and IDD consumers and families.
Event Description
North Carolina’s public Behavioral Health and Intellectual and Developmental Disabilities (I/DD) System is undergoing major changes. We want to hear from our consumers, families and advocates about how the system is working and how we can assist in creating a system that improves health outcomes and promotes recovery for all North Carolinians.
UNC-TV and the Governor’s Institute are hosting a series of webinars to talk about the changes and gather feedback from stakeholders in their specific local management entities/managed care organization (LME/MCO).
We want to include your questions at the end of the webinar. You can post your questions in the live chat during the webinar or you can record a video message beforehand and upload the video file to a OneDrive folder we have set up for the meeting. You can also email your questions to Suzanne.thompson@dhhs.nc.gov, but please include the LME/MCO in the subject line. To upload a video of your questions, go to the “Upload Your Video Questions” link below.
All upcoming webinars start at 6 pm and can be accessed by going to the NC Governor’s Institute Facebook Live page at the time and date of the event.
More information about past and upcoming Virtual Town Hall Meetings for Behavioral Health and I/DD.
Event Description
Committee Meeting
These meetings will occur weekly until further notice.
Join Microsoft Teams Meeting
Event Description
Committee Meeting
These meetings will occur weekly until further notice.