
Programs closing
This story about the impact of COVID on the treatment industry grabbed my attention:
At the beginning of 2020, addiction treatment was a solid, growing industry, with 15,000 providers, $42 billion yearly revenue, and a projected 5.2% annual growth. Then Covid-19 hit.
By the summer, the industry had lost $4 billion in revenue, and about 1,000 providers—and that’s just the beginning. According to the latest survey of the industry, published Sept. 9 by the National Council for Behavioral Health (NCBH), which represents about 3,000 mental health and addiction treatment providers, 54% of organizations have closed programs and 65% have had to turn away patients. As a result, nearly half have decreased work hours for staff, and over a quarter had to lay off employees.
My first reaction was ambivalence–there are a lot of bad actors and profiteers in the industry, maybe this will push some of them out.
Not so fast.
While a majority of rehabs have been hit hard, there is a specific group that is already seeing the effects of increased demand: High-end services. These programs have luxurious settings and amenities, and fewer patients, which makes it easier to prevent possible exposure to Covid-19. “We provide premium services, and that’s been the saving grace in this,” says Tieman.
His organization’s three premium programs—two in Pennsylvania, and one in Florida—have stayed at capacity through the pandemic, he says, because patients with the financial wherewithal to check into a premium residential treatment programs have continued to do so as they face a greater risk of substance abuse. Compared to the general programs, which costs $35,000 per month and is typically paid for with a combination of insurance and financial aid, the premium programs are $75,000 a month, with no discount offered, and though they have fewer patients, the programs have been helping the organization minimize the losses through the crisis.
Worse yet:
Many smaller providers have struggled to keep their businesses going, and in some cases, have shut down entirely. This is especially true for facilities funded primarily through public insurance, which have a harder time getting sustainable reimbursement rates and were already in the most tenuous shape prior to the pandemic. These are providers that tend to serve the most financially vulnerable.
While these programs get a lot of attention for quality issues, many of them do provide quality services and function as important safety nets for our most vulnerable community members.
Growth sectors
While we witness the demise of some portions of the industry, there have been changes to increase access to other types of care–primarily telehealth and buprenorphine prescribing.
Godinez’s process was almost impossibly simple: She texted her doctor and a drug counselor, who briefly evaluated her via FaceTime and wrote a prescription that she filled at a Walgreens around the corner from her Hendersonville, Tenn., home — a process that, until March, would have been largely illegal.
…
Now, as they wield unprecedented freedom to prescribe addiction drugs by telemedicine and evaluate patients by phone, many doctors and advocates say they’re unwilling to relinquish that flexibility without a fight. Already, there is a burgeoning movement to keep many of the new policies in place permanently. Many treatment providers across the U.S. have said publicly that the new status quo represents long-sought change that could positively transform patient care for decades to come.
“You can’t put the genie back in the bottle,” said Stephen Loyd, a Tennessee addiction doctor who treated Godinez and who once served as the state’s drug czar. “This is how it needs to be — always.”
The pandemic is also amplifying calls to eliminate the “X waiver” that requires physicians to receive 8 hours of training before prescribing buprenorphine to treat opioid use disorders.
Due to the COVID-19 emergency, the US federal government has temporarily waived the initial in-person assessment for initiation of buprenorphine and has increased flexibility for the dispensation of take-home methadone. These changes allow prescribers to initiate buprenorphine treatment remotely. These changes are welcome, and the federal government should do more along these lines. All providers with prescriptive authority should be allowed to prescribe buprenorphine, which could be achieved by removal of the requirement for a US Drug Enforcement Administration ‘X’ waiver. Emergency funding for buprenorphine and methadone should be released so that patients who are unable to afford these treatments, particularly in states without Medicaid expansion, can access treatment. Importantly, the structure of treatment settings themselves could increase infectious spread without thoughtful redesign. Limiting requirements for frequent in-person visits, facilitating remote healthcare delivery and providing these healthcare providers with appropriate protective equipment would be paramount to preventing the further spread of SARS-CoV-2.
The regulatory context
Meanwhile, I was talking with a friend who works for an FQHC (Federally Qualified Health Center) about their substance use disorder services. They have a fairly robust MOUD service, prescribing a lot of buprenorphine and some extended-release naltrexone.
I asked about other services for addiction. He reported that they are unable to provide addiction treatment because they are not licensed for it.
Let that sink in.
The hurdle for prescribing buprenorphine is an 8 hour training for the prescriber (24 hours for nurse practitioners and physician assistants). For outpatient group and individual counseling, it’s licensure as a specialty program.
Further, we’re seeing the implementation of higher regulatory standards for addiction treatment. This is in response to quality problems in many programs. It’s not a bad thing, if done properly.
So, we got a push for the deregulation of medications for opioid use disorders (MOUD) and a push for increased regulation of other forms of treatment.
Should we care?
As this blog has pointed out over the years, diversion of buprenorphine is a reality.
Most advocates quickly respond that illicit use of buprenorphine is for non-medical self-treatment and avoidance of withdrawal by people with opioid addictions. Further, that this is proof that buprenorphine is over-regulated.
A recent story in Filter explores the emergence of buprenorphine misuse by people who were not previously or currently using other opioids.
There has been an abundant market for Suboxone on the streets of Kensington for several years, as I’ve reported for Filter. And some municipalities, including Philadelphia, have begun dropping criminal penalties for possession without a prescription. But until recently, I had never met a Suboxone user who didn’t previously or concurrently take another opioid.
...
The reasons for its emergence are complex, but a significant factor is the ease with which Suboxone, thanks particularly to its sublingual film form, is smuggled into jails and prisons—and then concealed and divided once inside. Together with synthetic cannabinoids (called “deuce” on Philly street corners), Suboxone is anecdotally the favorite drug in Philadelphia County’s carceral settings.
…
Once inside, the strips are cut into smaller pieces which are taken orally, or else dissolved in water and snorted. The euphoric effects of buprenorphine on a person without opioid tolerance are indistinguishable from other prescription opioids. Regular use can lead to physical dependency. So released people, as they have recently described to me, have been returning to the streets with a taste for the orange films, which are sold up and down Kensington Avenue and on street corners across Philadelphia.
A more scholarly look at non-prescription use of buprenorphine found that the most commonly cited reasons for non-prescription use were self-treatment and avoiding withdrawal. However, more than half (52%) of respondents reported using it to get high.
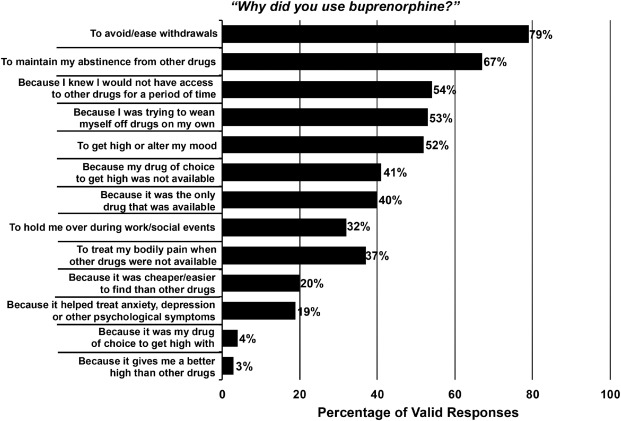 Cicero TJ, Ellis MS, Chilcoat HD. Understanding the use of diverted buprenorphine. Drug Alcohol Depend. 2018 Dec 1;193:117-123.
Cicero TJ, Ellis MS, Chilcoat HD. Understanding the use of diverted buprenorphine. Drug Alcohol Depend. 2018 Dec 1;193:117-123.
While it hasn’t been widely reported, this has been known for years. My first post on the problem was in 2006. Further, failure to acknowledge the problem has the potential to create serious barriers for many people with addiction seeking recovery. For example, mandates that all recovery homes allow opioid agonists like buprenorphine. (Those SAMHSA guidelines were not mandates, but mandates have been discussed at the state and regional levels. The first step is making funding of services contingent on integrating opioid agonists into all housing programs.)
What we miss when we focus on opioid treatment and recovery
(This section is a post from September 17th, 2019)
Fortunately, there’s been growing concern that advocates, policy makers, and media have to narrowly focused on the opioid crisis. Up to this point, it hasn’t reached the level of media coverage.
USA Today is one of the first to publish an article that explores the limitations of the nation’s focus on opioid treatment and recovery:
More than eight years into his opioid-addiction treatment, Paul Moore was shooting cocaine into his arms and legs up to 20 times a day so he could “feel something.”
The buprenorphine he took to quell cravings for opioids couldn’t satisfy his need to get high. Moore said he treated himself like a “garbage can,” ingesting any drug and drink he could get, but soon enough, alcohol and weed had almost no effect unless he vaped the highest-THC medical marijuana available.
Cocaine, however, especially if it was mainlined — now that could jolt him from his lifelong depression to euphoria.
The article provides several important messages:
- The importance of addiction treatment over opioid use disorder treatment for many (if not most) patients.
- Along similar lines, messages about opioid recovery can be misleading for patients, families, and communities.
- These issues raise the importance of clarity about the boundaries of recovery. For example, were these people in recovery when they were in opioid use disorder treatment and reduced or quit using opioids, but were still using cocaine and experiencing poor quality of life due to untreated addiction? (This would have been an uncontroversial and easy question to answer just a few years ago. Today, there are many saying that any movement toward wellness or participation in harm reduction is recovery.)
- The article also highlights what gets missed when agonist treatments (buprenorphine and methadone) are described as the most highly effective and highly successful treatments without more context. They rarely answer the question, effective at what? (This isn’t saying that these medications aren’t useful or don’t have a place in care. Rather, it’s important that journalists and experts do not oversell their evidence for effectiveness.)
Failure to clarify and communicate these messages are likely to result in increased stigma for addiction and recovery.
Rather than communicating that addiction is a treatable illness, the unintended message will be that addiction more closely resembles a chronic disability than a treatable illness that has a good prognosis when the patient receives treatment of adequate quality, duration, and intensity.
This century’s first wave of recovery advocacy was built upon the message that we can and do recover when we get the right help and support. In this context, recovery meant something resembling the Betty Ford Consensus Panel definition:
Recovery from substance dependence is a voluntarily maintained lifestyle characterized by sobriety, personal health, and citizenship.
The traditional understanding of addiction recovery alludes to the restoration of people in their families, communities, and to a life in alignment with their goals and values.
Adjustments to that understanding are likely to result in readjustments in the public’s attitudes, which are eventually likely to result in readjustments in policy.
Thanks to Treatment Magazine for the story about us. You can find it here.

Churchill famously said that the US and Great Britain are two countries separated by a common language. Arguably TV and movies may have bridged the divide a bit, but nuances of language and spelling are not the only things that differentiate us; something I was aware of when reading Marc Galanter & colleagues’ paper on the construct of ‘God’ in 12 step recovery settings.
The first thing in the paper that struck me was the percentage of the general American population who believe in God (89% vs 60% in the UK). In the study population (450 US Narcotics Anonymous members), this God belief was slightly higher still (91%). Now I don’t know for certain, but I’m pretty sure that figure would be much lower here in the UK.
The question might be forming in your mind as you read this – so what? Well, in my experience here in Scotland, one of the commonest reasons that professionals are reluctant to refer into AA, NA or CA is that ‘God’ word. Indeed many patients here are also hesitant or downright opposed for the same reason. If you have a population where belief in God is much lower, the odds are there will be more resistance.
There is reason to be much more hopeful, however, as this paper shows. In a nutshell, the authors (big names in recovery research) recruited the NA members through cooperation with meeting organisers across 34 meetings in 9 separate states. The the vast majority of meetings attenders completed the survey forms.
It turned out that ‘belief in God’ was more nuanced than might initially have been thought. Less than half of the NA members surveyed actually defined ‘God’ as explicitly ‘God’, if you see what I mean, and slightly more than half believed in some other entity. About 1% in one section of the survey identified as atheist, though in another section 17.4% said they were agnostic and 3.5% said they were atheist. I read this as some fluidity in definition and belief.
The authors looked at the relationship between what they called ‘antecedent 12-step items’ (things like how many steps had been worked, whether a life had been ‘turned over to God’ etc.) and symptoms of craving and depression. The findings were in line with previous research that showed an inverse relationship between these negative symptoms associated with addiction and with spirituality.
What was interesting, if I’m reading this correctly, was the finding that it didn’t matter if you explicitly believed in God, believed in some other entity or didn’t believe in God at all – the association with improved symptoms was still there.
The authors said:
The finding that there was no difference in certain key variables across respondents suggests a broad bandwidth of tolerance and accommodation to varying viewpoints.
What this means is that there’s plenty of evidence in flexibility of belief in Narcotics Anonymous. This can give referrers a bit of reassurance. With the recent Cochrane review of the evidence for the impact of getting people along to Alcoholics Anonymous (at least as effective as other evidence-based interventions), then all of us working with people seeking recovery can have confidence that a breadth of perspectives and beliefs can be accommodated in 12-step mutual aid groups.
The authors also say:
The cost-free resource of 12 Step groups may be potentially useful to clinicians as adjuncts to care if they can assure their patients that there is a diversity of options in how members define God, particularly given the growth of secular wings within 12 Step fellowships created by and for atheists
Many clinicians may therefore be making less use of 12 Step groups than they might, witness the fact that 65% of the respondents had been hospitalized for SUDs, but only 37% of them had been referred to NA by a health-care professional.
And then:
The cost-free resource of 12 Step groups may be potentially useful to clinicians as adjuncts to care if they can assure their patients that there is a diversity of options in how members define God, particularly given the growth of secular wings within 12 Step fellowships created by and for atheists
It seems that even for us heathen Brits, there is hope.

[Chris Budnick did this interview with West. Thanks to both of them!]
Who are you?
My name is Darryl West, and I just go by West. I’m a person in long-term recovery, and I also work in the field treatment.
What do you do professionally?
Professionally, I am a certified substance abuse counselor here in the state of North Carolina. I work for the Department of Public Safety within the Department of Adult Corrections, I work for the Division of Alcohol and Chemical Dependency Programs, and I wanna say as a disclaimer, I do not speak on behalf of the ACDP [the Alcohol and Chemical Dependency Programs]. I’ve been working with them since 2005, so over 15 years. We provide SUD services for offenders within the Adult Corrections.
Do you have any personal interest in addiction and recovery that you’d like to share
Like I said, I’m a person in long term recovery. I’ve been in recovery since January 24, 2001, so that’s 19+ years. Personally, [addiction has] affected my community. I have a brother that has even more time in recovery, some other family, some friends. So yes, I have definitely been personally affected. I’m also fortunate to have found recovery and to have received treatment services that led me to the recovery process.
Tell us about your professional experience in the area of addiction and recovery
I got into the field through my own personal treatment. I guess as a safeguard to continue my treatment, I started working or started working at The Healing Place (now known as Healing Transitions), in the detox and shelter area. At the time, I didn’t realize I was performing some of the core functions of addiction counseling. Later, I went on and got some courses and got deeper into the field, and I think I got certified in 2009.
I’ve worked with women, men, and youth, in detox services, inpatient, outpatient, with different modalities, Minnesota Model, and CBT. I’ve stayed actively involved professionally, as much as I can.
I also worked with Southlight for a while, doing some ADETS [Alcohol Drug Education Traffic School] classes.
Professionally, what are you most proud of?
West: I don’t know who he or she is that I’m most proud of, but I’m sure there is some child or grandchild who has been touched by something that I’ve shared with one of their parents, or relatives, or friends. Something that had a ripple effect, helping them have a more whole life because of it. I think that’s what I’m most proud of–the unknown of who might have been touched by what I was given to give to them.
What keeps you working in addiction and recovery?
What do they say about insanity? Haha.
It’s just fulfilling. Is there anything else to do, but give back? I’m sure there are other forms of service that we can give to our community, to our country, to our families. I just found this is my niche.
I didn’t plan to do this as a form of service or even a plan of employment, but it’s something that is fulfilling… that you can’t buy it, you can’t find it in headlines. Yeah, I’d like to play in the NBA or be a comedian, or be a music star, but this is where I was meant to be.
I don’t fight it and I don’t force it. It just works naturally.
How has the pandemic affected your work?
First of all, I want to say it has affected my work and me personally, but let’s go with work.
Nobody was prepared for this… many people have suffered… many people are still dealing with it and trying to cope.
I’m fortunate that I have work, I haven’t lost a minute of work since February, March, whenever this thing was declared… but how has it affected my work?
I work at a maximum security women’s prison.
At the beginning of the pandemic, we had over 1500 women at the prison. I think we’ve reduced our census greatly, for a lot different reasons. For example, all the pregnant females were released or moved.
I work in an outpatient program, which sounds funny for a prison. We have 102 women, in a four to six month program, where women receive services Monday to Thursday, and we try to give them in a minimum six hours of programming–group, one-on-one, skill building, and recreational.
Since the pandemic started, of the 1500 women that are assigned to the facility, we’ve found over 270 known positive cases among the “inmates” and many of them were in treatment at the time. (We call our clients “clients.”)
In March, we tried some preventive measures and safety measures, of course, but the women weren’t really receptive to the restrictions (or guidelines) that were presented to them–as far as wearing masks, social distancing, hand washing, on and on. It is pretty hard in a facility of that size without the space to provide some of those essential needs to stay safe from the virus.
We started implementing precautions by making our groups smaller. We normally have 102 women and six counselors, so each counselor should carry a caseload of approximately 17 people. At present, my caseload is down to 5 people. That’s from people getting released. I think our total census is down to maybe 34 or 35.
So, in March, we went with some preventive measures, but at the end of June, we went to total lockdown at the prison, which meant there was no movement. Our clients started receiving their food in the dorm. They weren’t allowed out 24 hours a day. They were locked down from, I believe, June 30th until maybe the end of August. There was no movement. They didn’t come out, they didn’t move.
They live in a quad, with 34 or 36 women to a quad. It was repressive. I’m sure that they’re still recovering. They were suffering. There was no air conditioning or fans. They were just locked in there all day–no recreation, no time out, no matter what.
Of course, that limited treatment services, they couldn’t come to us for services.
Like I said, we’re an outpatient, but what that means is they live in their quarters, but they come up to our building and we provide the services, groups, and so forth.
We were sending assignments to them… but is that really treatment? Or, is that just sending the assignments? And, we didn’t collect the assignment because of course, we didn’t want cross-contamination from the paperwork or the books.
It has really affected the women. There’s no physical contact within a group… no touching one another… no being in a group setting… not even one-on-ones with the counselors… they can’t do treatment plan updates.
I haven’t done an assessment on a client since March or April because I haven’t gotten any new clients, so we’re not putting people into treatment. So, the whole program has definitely been shut down.
People are getting released, so it’s not like they’re put on a waiting list or in a holding pattern.
But, here’s the weird thing, when you’re in a North Carolina prison, and if you’re assigned to certain programs or services, you get what they call gain time. So you can be in treatment for 30 days and you might get, let’s say, four days off your sentence. They’re still receiving this gain time, which is great, but are we setting them up? Will they have the proper tools for when they do return society, and return to their normal situation?
It’s also affected us as counselors and me professionally. We are still receiving virtual clinical supervision from my supervisor. We do monthly trainings. We still have staff meetings, and we still try to staff clients, to go over their needs and preferences, and wants. So now I might see my clients maybe five, six minutes a day. Services like setting up aftercare plans, and home plans, and transitional services for when they do release is limited.
It has definitely put a burden and a hindrance on the program that I’m in. There are other programs within the prison system that are up and running because they didn’t have the magnitude of virus in their facilities, so it has definitely impacted the services that we can provide.
I know that’s a lot, but there’s a lot that needs to be heard.
What, if any, long-term effects do you anticipate on the field?
It’s weird, we’ve got plans for everything but a pandemic. When you talk about a prison and state government… they have countermeasures for countermeasures for countermeasures. There were no countermeasures for something of this magnitude.
I think we’re definitely gonna have to reduce group sizes. They say a good group is what… maybe 10 to 12 people… we might even have to look at 6 to 8 people as an effective group size. Spacing, of course, is gonna be important.Simple hygiene, and not just HIV and AIDS, but other hygiene training and services and information, that’s gonna need to be passed on the clients and staff. How does the staff [protect themselves]? We’re not immune from contraction.
Also, how are we going to provide services virtually? Is there an effective way to provide virtual treatment services? That’s a hard one, because this is such an insidious disease. Addiction is so weird, that people sometimes need the feeling of feeling… not just touching, but feeling… and sometimes virtual can be sort of cold and… I don’t know… it just seems distant.
It’s weird, I remember my daughters being in the back seat of the car and texting each other. I would be like, “what in the world?” But maybe that’s the world we’re moving to. I just can’t get it.
I like to be around people. I like to feel people. I like to hear people. I like to smell people. Some of the dynamics of treatment are definitely going to have to be readjusted. Even, you know, the lights of the room, the color of the room. You know, do I put a false backdrop when I’m doing virtual work from home? Do I put up waterfalls and butterflies? Or, do I keep it real and just have a bare white wall?
I guess there’s a lot of things that we’re gonna have to look at as professionals.
Have you seen any benefits or new opportunities in the pandemic?
Like I said, there are definitely improvements in hygiene.
A lot of people like to hug in this field… that touch, that feeling of being connected, that heartbeat to heartbeat type thing has sort of diminished. But, I’ve also seen that people care about each other. It also brings out that humanness. How many times do we hear people say, “Now, stay safe, be careful”?
It also brings out the sense of selflessness. I think the pandemic has definitely brought out a sense of caring about somebody. We know that the core of addiction is self-centeredness. I think one of the things that the pandemic has brought about is a momentary lapse of that selfishness. We’re concerned about others, we’re concerned about straightening up or cleaning up behind ourselves a little more. We’re not just assigning it to the janitor. People are more mindful… we are more aware of our surroundings and aware of other people.
But also, somebody can have a normal sneeze and everybody freaks out.
If you were able to work on a fantasy project to improve treatment and recovery support, what would it be?
Well, I’m gonna go from my experience and my arena of where I work. Women, and men, do well in prison treatment services. We follow it statistically and they have less recidivism. They have fewer infractions while in treatment services. They also say that even once they complete treatment services and are reintroduced to the regular population that their infraction rates go down… definitely, their violent infraction rates go down.
So, they do well in prison and they do well in treatment, but the big gap is transition.
On the outside, we’re getting all these treatment high schools. One day it’s going to be great when we have Recovery University (you know, like Liberty University) we will have Recovery University.
So, my treatment fantasy would be a do-all treatment facility for criminals, where they serve their time in a dedicated treatment facility. NOT a unit in another facility, but a dedicated treatment facility. Then, during their transition period, sanctioned by the state, they get treatment services, mental health, social work–throughout that transition period as part of their sentence.
I think that would be my fantasy. That’s the treatment that I would want for a person that has to pay their debt to society, but also has the chance to live in a recovery safe zone–even in prison. That’s what I would try.
Minority Fellowship Program for Addiction Counselors
Applications due December 15
Are you committed to providing additions counseling services to underserved communities? You may be eligible for one of 40 master’s-level counseling fellowships through the Minority Fellowship Program (MFP).
NADCP is pleased to inform you, the National Board of Certified Counselors (NBCC) and the Association for Addiction Professionals (NAADAC) are now accepting applications for the 2021 National Board for Certified Counselors Minority Fellowship Program for Addictions Counselors (NBCC MFP-AC). The program, funded by the Substance Abuse and Mental Health Services Administration, provides up to 40 master’s degree-level counseling fellowships of $15,000 for addiction counseling students, travel expenses to participate in program-related trainings, and complimentary NAADAC membership.
Applications are due by December 15, 2020.
The post Minority Fellowship Program for Addiction Counselors appeared first on NADCP.org.

Imagine this scenario. You get the terrible diagnoses of cancer, like addiction, it is terminal if left on its dreadful course unimpeded. You are in the depths of despair, facing everything this terrible diagnosis means for your life.
The treating professional turns to you and says “recovery is possible. It is POSSIBLE you might survive this, it does HAPPEN.”
I would not be reassured by such a scenario, and the truth of the matter is that people beat cancer every day. This is a result of an advancement in science, a commitment to fund care and a dedication to follow multiple pathways of care, people who get that diagnosis survive. This occurs because the care team never gives up and keeps working until they hit on the combination of care needed for the person to move into remission. In respect to cancer, the truth of the matter is that the death rate from cancer in the US declined by 29% from 1991 to 2017. This occurred in large part due to a commitment to study outcomes over the long term and to fund care. What this means for a person sitting in the chair learning that they have cancer is that the treating professional knows which treatments have the best chances of getting you into and sustaining them in remission for five years. They also know that there is wide variation in what works for whom. This means that they use multiple treatments and combinations of care to achieve remission
We know that addiction recovery is a probable outcome given the proper care and support they need 85% of the people who stay in recovery for a period of five years stay in recovery for the rest of their lives.
Let’s start using more accurate language:
Recovery is the probable outcome for people with substance use disorders when they provided proper care and support.
We need to focus on long term recovery as our focus of all addiction policy. Let’s study long term recovery and support multiple pathways and service strategies. Let’s do a moon shot, national focus on recovery so that in twenty years we can say that we reduced deaths from addiction dramatically, just like we did with cancer.
That starts with framing our discussion with the proper language of recovery as the probable outcome when people get what they need to get to get better and acknowledging we are a long way from achieving a system that provides that focus for all Americans.
So please stop saying recovery is possible and let’s focus on recovery being probable if we move towards recovery focused policy so we change our care systems to reflect the needs of persons seeking help with a substance use disorder.

The SMART Community had the opportunity to hear from Board President Bill Greer and Executive Director Mark Ruth as they shared their perspectives on what the SMART community has accomplished in 2020 and where we are headed in 2021.
Watch this video on our YouTube channel
Support SMART’s Recovery Month Fundraising efforts
Download the PowerPoint presentation
Subscribe to the SMART Recovery YouTube Channel
Video storytelling is a powerful tool in recovery, and we are proud to share our SMART Recovery content free-of-charge, available anywhere, on any device. Our videos hope to inform, entertain, and inspire anyone in the recovery community.
Subscribe to our YouTube channel and be notified every time we release a new video.
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!
This post was originally published on September 27, 2015.
This post focuses on an article critically examining the use of recovery as an outcome measure by professionals. They distinguish between recovery as a process (an individual journey rather than a specific outcome – a deeply personal experience related to one’s life goals, needs, and striving) and recovery as an outcome (a cure – a complete absence of symptoms of illness and/or a return to premorbid functioning – rather than as developing a satisfying life in spite of symptoms or vulnerability).
 Pat Deegan (with Robert Drake) published a recent article on measuring recovery as an outcome. Their focus is on mental illness, but it offers some interesting food for thought about parallels with addiction recovery outcome research. As access to care grows, an important question is whether actually facilitates recovery.
Pat Deegan (with Robert Drake) published a recent article on measuring recovery as an outcome. Their focus is on mental illness, but it offers some interesting food for thought about parallels with addiction recovery outcome research. As access to care grows, an important question is whether actually facilitates recovery.
Perhaps we can measure some of the processes corresponding to the recovery concept: More people with serious mental disorders have the freedom to live outside of institutions, avoid medications and coercive mental health systems, and pursue employment, friendships, and love relationships in their communities. These are measurable variables. Yet recovery processes are clearly compromised by the ubiquitous problems of poverty, lack of safe low income housing, dangerous neighborhoods, victimization, constant threats of coercion (sometimes by the criminal justice system as well as the mental health system), stigma, the lack of educational and employment opportunities, and the dearth of evidence-based interventions that could enhance functioning.
The evidence that recovery outcomes are improving is minimal. One of the most widely assessed recovery outcomes is competitive employment – a primary goal for the majority of people with serious mental disorders. The evidence shows that employment remains very low (under 20%) (60–61) and has actually decreased during the recent recession (60,62) because people with disabilities suffer greater job loss during recessions (63).
Raising awareness of the recovery concept has not actually improved positive outcomes; current measures of recovery fail to capture the process concepts and individual goals that inspire service users; and generic recovery measures cannot assess personal goals, diversity of populations and programs, and cultural context. What should be done?
Disappointing. Especially since every provider identifies their services as recovery-oriented. They offer an interesting response. They step back to reassess. On the one hand, the push for recovery-oriented services may result in simple re-labeling of approaches. And, quantitative quality of life measures can incentivize interventions that don’t feel like recovery to the client. On the other hand, the pushing of recovery measures, while imperfect, may at least help broaden the focus of providers.
Perhaps we should accept that recovery is a personal journey – a concept developed and owned by people who have lived experience – and avoid co-opting the term to advance professional, program, research, and system goals. If recovery is indeed a process, perhaps the mental health system should focus on measuring positive and negative outcomes (both are important) without asserting that some are recovery outcomes. But processes are also critical. Focusing on outcomes exclusively may devalue the ideals and the process issues that are important to users of the mental health system and may lead to manipulations to show good outcomes despite poor processes. For example, placing people in work enclaves for jobs that do not match their interests achieves high employment rates but violates the process goals of choice, self-determination, and quality of life.
Perhaps we should accept the problems and complexities of measuring recovery and continue to operationalize processes and outcomes that are consistent with recovery. Recovery is an inspiring ideal, and programs need to assess the outcomes that align with recovery as well as with their goals. Labeling some outcomes as recovery may at least help program managers to select outcomes that are important to participants. For example, people with mental health symptoms clearly advocate for safe housing, jobs, and quality of life – all measurable outcomes – rather than medication compliance.
Perhaps genuine attention to recovery outcomes could help professionals to understand processes and goals that their clients value and also recognize that clients need to be centrally involved in developing and assessing programs. Inclusion would be consistent with the principles of community engagement research (64) and might lead to innovative approaches to developing services and assessing their success. For example, programs that empower people to make decisions about life-goals and treatments may facilitate self-management. One method of doing this would be to distribute electronic self-management systems and self-referral systems directly to people with disorders. Users of mental health services could then select the services they want (65–66).
Perhaps involving clients in measuring processes and outcomes might deter professionals from relabeling traditional clinical approaches, such as case management, skills training, and medications, as recovery-oriented. Instead, programs might develop and implement services that people truly want: services that emphasize financial, residential, and personal independence; normal adult roles such as education, employment, home ownership, and intimate relationships; and personal choices regarding treatments and illness management.
I’ve written frequently about the need for an increased emphasis on quality of life measures rather than building an evidence-base grounded in measures of reduced drug use, reduced crime, reduced disease transmission and reduced OD.
It’s interesting that they see themselves as grassroots advocates seeking to overcome deeply entrenched professional interests that emphasize medication as the primary tool and medication compliance as a primary outcome measure.
Simultaneously, in addiction treatment, we’re seeing professional and institutional advocacy to increase use of medication. These advocates see themselves as seeking to overcome deeply entrenched grassroots and grassroots-rooted professional interests that are skeptical and resistant toward medications. (Believing that the effectiveness of treatment medications are overestimated, that they may undermine goals of recovery, that their PHARMA’s bad behavior makes them untrustworthy, and that medications have a tendency to become treatment rather than treatment tools.)
This article does a great job laying out the mental health experience and some important questions that we need to attend to as our field changes in ways that will be for the better and ways that will be for the worse.
This post shares a few loosely connected tabs that have been open in my browser for a couple weeks.
An advocate’s sad end
Over the years, I’ve expressed concern about peer supports being placed in high risk situations with inadequate training, supervision, and support. My concern has grown as the OD crisis has accelerated, along with the use of peer supports on the frontlines of this crisis.
My concern has typically centered on people in the first months and years of their recovery being placed in environments and relationships involving regular exposure to drugs, cultures of addiction, trauma, etc. Peers are often the addiction professionals with the least training, supervision, structure, and institutional support. Because the onramp to being a peer is short, they are also often in early recovery.
Stories like Jesse Harvey’s are the kind I had in mind. It sounds like Jesse ran some recovery homes that, at first glance, look like decent programs. It was his harm reduction work–The Church of Safe Injection–that got him some national attention.
Of course, workers in recovery-oriented treatment settings sometimes relapse and OD too, but there are expectations of internal and external structures to support, guide, and protect workers.
From afar, Jesse Harvey’s work was interesting to me because he seemed legitimately inhabit both worlds–recovery and harm reduction. (I’m aware that many see no need to distinguish between the two.) It is sad to see his story end this way.
For me, it’s been important to distinguish between harm reduction as an approach to working with and engaging people who use drugs and harm reduction as a philosophy. I wonder if that distinction can serve as a protective factor for people in recovery. I don’t know, just a thought.
‘Peer’ work as precarious
A paper entitled ‘Peer’ work as precarious recently caught my attention. I imagined it was about the risks peers in recovery (recovery coaches) might encounter.
I was mistaken. It’s about the experiences of peers who currently use drugs.
They interviewed 15 peers who use drugs and work in harm reduction services.
One might imagine that people-who-use-drugs who are hired, as people-who-use-drugs, to help other people-who-use-drugs, would find that experience validating. This isn’t the case for the subjects of this paper.
Instead, the paper described the subjects’ reports of feeling exploited. This is one of the four themes explored:
Peer workers lacked access to workers’ rights and were unaware of what their rights included. Nonstandard arrangements systematically constrained access to rights as there was no formal employee-employer contract. Some said: “there’s no rights” ; and “[peers] have no rights”. These perceptions were concerning but reinforced by the numerous violations to provincial workers’ rights reported by participants, including wages that were below provincial minimums, a lack of social benefits (i.e. sick and vacation pay), physical and verbal intimidation, and no access to safety standards. Another participant shared a unique perspective on the lack of access to workers’ rights: that they were a PWUD.
“There’s also the question of drug use at work and how that impacts people and that’s one of the reasons why people get paid so less or much less…. if people are using drugs at work it’s, like, okay, fine, you can use drugs. But you’re not going to have any workers’ rights or be paid a basic wage type of thing.“
Negating workers’ rights was seen as necessary in a work culture that tolerated PWUDs substance use needs. This quote underscores the structural vulnerability of PWUD produced from the criminalization of drug use – even in harm reduction work.
Model for drug policy?
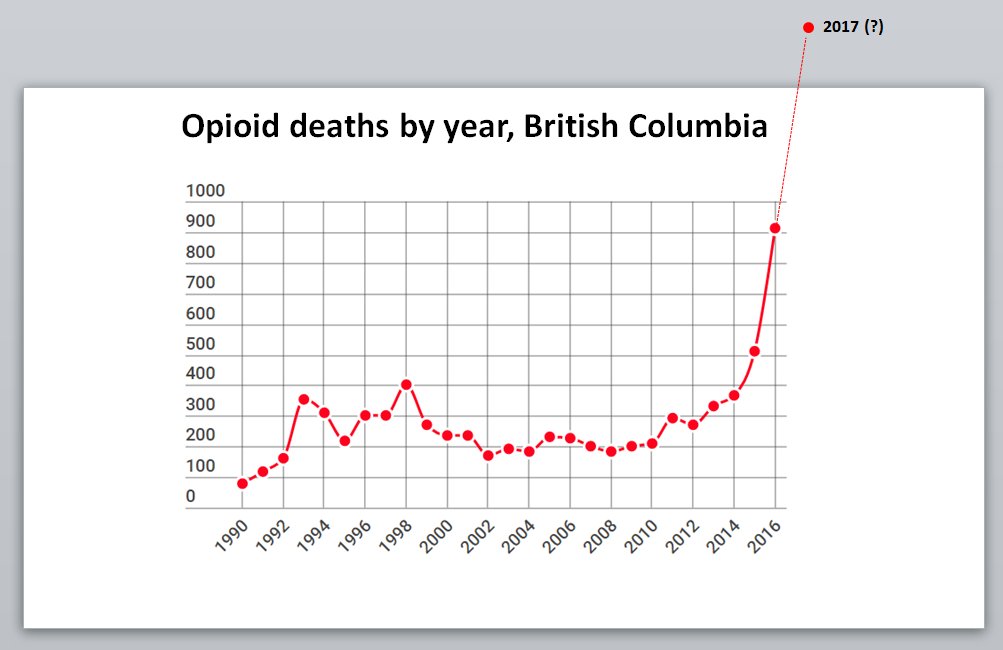
British Columbia (BC) and Vancouver have been touted for having model drug policies for 2 decades. This blog has followed their drug policy for most of that time.
BC and Vancouver are at the vanguard of harm reduction policies and the experiment does not appear to be the success that many hoped for.
From CBC:
British Columbia has nearly matched its monthly record for deadly illicit drug overdoses, with 175 deaths during the month of July.
The BC Coroners Service saw 177 fatalities in June, which surpassed the previous high of 174 deaths in May. The service initially reported 175 deaths for June but updated the number on Tuesday.
A statement said the service has detected “a sustained increase” of illicit drug toxicity deaths since the first peak of the pandemic in March, and it’s now confirming five straight months with more than 100 such deaths.
The proposed solution? More harm reduction:
Medical leaders, physicians and advocates speaking Tuesday all called for the same measures to save lives. They pushed for decriminalization, a safe supply for users and erasure of the stigma surrounding substance use.
“Given the toxicity of the drug supply, now is the time for all of us to demonstrate compassion and empathy,” said Lapointe.
Communities that haven’t embraced harm reduction are struggling too and there’s no doubt that the pandemic has interfered with access to both harm reduction and treatment services, but it’s clearly not just the pandemic.
 See: Overdose crisis? Or, addiction crisis?
See: Overdose crisis? Or, addiction crisis?
To me, the problem isn’t the interventions being used. It’s the absence of attention to treatment and recovery. The words “treatment” and “recovery” appear zero times in that article. There isn’t even mention of opioid agonists, just access to a safe supply of drugs.
This is where I get uncomfortable with harm reduction as a philosophy rather than a set of strategies/interventions. Harm reduction isn’t enough. (Treatment also isn’t enough. Too many people will die or get a chronic illness before achieving stable recovery.)
Seeing this through the philosophy of harm reduction leads people to framing this as a problem of toxic supplies and people using alone, rather than seeing it as an addiction crisis and seeking ways to better treat that illness–as though we’d want that life for a loved one… if only they had a safe supply and a using buddy.
This is the second in a series of interviews of people in and around the Recovery Space.
- Who are you?
My name is John Winslow and I am a person in long-term recovery. For me that means that I have not used alcohol or other substances for over 44 years. I’m what we refer to as a “Snowbird”. My residence is in Bradenton, Florida on the beautiful Gulf Coast, but I spend my summers “up North” at Virginia Beach, Virginia during the hot season. I’m married with a daughter, a son, and three grandchildren.
I had just turned 26 years old when I entered into recovery. At the time I couldn’t imagine a life without alcohol and other substances. I was what some might refer to as “a sick pup” and my life was a wreck. As a result of having had a great treatment experience and throwing myself into recovery, my life turned around 180 degrees. I shifted from self-loathing, shame, humiliation, remorse & regret, and despair to learning to love myself, gaining self-respect and the respect of others, and leading a life of love & service.
2. What do you do professionally?
I’m retired! However, that doesn’t mean that I simply spend all day walking along the beach looking for seashells and golden doubloons. Read on and I’ll tell you more…
3. Do you have any personal interest in addiction and recovery that you’d like to share?
Yes, I absolutely have a personal interest in addiction and recovery. When I first got sober, I realized that if I was going to maintain my recovery over the long haul, I would need to establish a career that would support my long-term goals. Through the process of prayer and meditation along with consulting with my recovery guides, I felt spiritually led to enter the emerging field of addiction treatment. At the time there were few young people in recovery working in the addictions field. I have always believed in the power of example. As people began to recover at younger and younger ages, I believe it was helpful for them to see someone with whom they could identify staying sober and living a life of service.
4. Tell us about your professional experience in the area of addiction and recovery.
My first job in the addictions field was as an evening counselor at Springfield State Hospital in Sykesville, Maryland. I left a good paying job with the Federal government to get my foot in the door as a neophyte counselor. The pay was so low that I was forced to live on the grounds of the hospital in a small one-room bedroom overlooking the psychiatric patients below, doing what we then referred to as the “Thorazine Shuffle”. It was a wonderful training ground for the rest of my career. I ended up returning to school, having had only a high school diploma. I obtained my master’s degree in Human Services and over time became a Licensed Professional Counselor. Having worked in a variety of settings, I eventually established and ran my own private outpatient addictions treatment practice for 20 years. In 2004, I relocated to Maryland’s Eastern Shore where I became the director of Dorchester County’s outpatient program and founded one of the state’s first recovery community centers: Dri-Dock Recovery & Wellness Center. During that time, I was elected president of the Maryland Addictions Treatment Council.
Over time, my focus and passion shifted from addiction treatment to that of recovery services and advocacy. I was recruited by the Maryland chapter of the National Council on Alcoholism & Drug Dependence as Coordinator of their Recovery Leadership Program. It was in this capacity that I expanded my growing interest in connecting the dots of recovering individuals, families, and communities which in time led to the creation of International Recovery Day.
5. What are you most proud of?
I would say that of the things that I am most proud is far and above – that of my continuous recovery. *in saying this I must note acknowledgement that my recovery was (and is) a gift ~ but I do take credit for the footwork that I’ve put into this miracle of miracles occurring in my life! As they say… “it’s a simple program, but it ain’t easy”.
On September 11, 2001 our lives changed. A few days later I sat in a classroom at Eagleville Hospital taking my examination for Licensed Professional Counselor. Immediately upon completing this grueling test I drove into New York City and landed at Ground Zero where I served with a Red Cross Mental Health team offering support to the police & firemen attempting rescue efforts.
Lastly, I’m proud of having established International Recovery Day, Inc. The premise is based on the concept that “We can do together what none of us can do alone.” We’ve created a global recovery event that embraces all addictions and all recovery pathways all on the same day!
6. What keeps you working in addiction and recovery?
I am driven and guided by my inner voice (which I identify as the God within). The world has suffered too much heartbreak and devastation at the hands of addiction. My hope is to shift the focus from the ravages of addiction to the hope offered through the recovery movement. We need to collectively demonstrate to the world that we can and DO recover.
7. How has the pandemic affected your work?
The Covid-19 pandemic has been devastating to addiction treatment and recovery efforts. Most Recovery Month events have historically been held in person. Unfortunately, many of those events were cancelled this year. Due to the fact that International Recovery Day is an on-line event, we were not hampered in that regard. There were a number of exceedingly large in-person events through which we had planned to inform recovery audiences about our event. Those plans had to be scrapped. However, we’ve attempted to take full advantage of social media to move our message forward. The other primary segment of International Recovery Day is our “Recovery Lights Around the World” campaign that has not been significantly negatively impacted by the pandemic. We have well over 80 structures around the world that are going purple on Sept. 30th, to include Niagara Falls, the Ben Franklin Bridge, Aloha Towers, and the Rock & Roll Hall of Fame, to name a few.
8. What effects of the pandemic are you observing in the people you serve?
We know that in addition to a significant increase in alcohol consumption within the general public and the reduction of services and closure of treatment programs… suicide, relapse, anxiety, and depression have all increased significantly as well within the recovery community. The recovery community more than ever needs to hold out a beacon of hope to those still in need of help and services. International Recovery Day serves to offer that beacon to the world!
9. What, if any, long term effects do you anticipate on the field?
As with other segments of our society, the pandemic is taking a significant toll on prevention, treatment, and recovery organizations, institutions, communities, and individuals. I’m mindful of catastrophe movies such a “Deep Impact” in which the survivors gather together afterwards clinging to the words of their leaders proclaiming the time for rebuilding is at hand. We of the Recovery Movement know all about surviving catastrophes and of rebuilding. We’ve rebuilt our own lives and lived through tough times – assured by those who came before us that “this, too, shall pass”. We need to have faith and take heart, to trust the process, but to also be prepared to grab a shovel and dig in ~ for there will be much work to be done.
10. Have you seen any benefits or new opportunities in the pandemic?
I am sometimes accused of being an optimist. I’m OK with that. I always believe that if we look hard enough, or step back, take a deep breath, and look at the bigger picture a vision of new possibilities will emerge. I continue to trust the process and look forward to seeing what is revealed.
11. If you were able to work on a fantasy project to improve treatment and recovery support, what would it be?
I really don’t need to envision a fantasy project for me to tackle. My Higher Power has already dropped it in my lap when upon reflecting on the words of William (Bill) White and a biography of Marty Mann the idea for a global celebration of recovery was revealed to me. On that day the concept of International Recovery Day was born. Our website: https://internationalrecoveryday.org/