
Faces and Voices’ blog has a new post arguing that social justice advocacy is in the recovery advocacy lane.
I don’t get to pick recovery justice outside of the frame of social justice because recovery justice is social justice. This doesn’t mean I need to be an expert on all social justice issues, but I don’t get to stay on the sidelines. Infringement of civil rights regarding recovery is no different than the infringement of civil rights based on race, religion, gender identity, sexuality, or ability. To act like we stand for one but not the other is at a minimum disingenuous, and worst-case scenario, supportive of systemic oppression.
While this might seem to some like a course change, I would argue that we’ve always been social justice warriors. The passion and energy I have seen regarding recovery issues is truly something to behold. We’re just widening the road a bit.
This is our lane!
Bill Stauffer recently posted here on the same subject, but didn’t share Phil’s certainty:
Decriminalization of drugs, social justice, basic human rights are all issues of deep, substantive concern for so very many of us, but are they our central focus? To what degree if any do we incorporate other issues of broad concern? What is in our “lane” and what is out of our “lane”? What do we risk if anything if we expend our energy on these other issues? I am not sure. But what I can tell you is that it does matter to me profoundly that we stay true to a common purpose and that purpose remains stronger than issues that would otherwise pull us apart.
I’ve recently have frequently found myself frustrated with discourse around nearly everything — COVID, elections, school and business re-opening, social justice, recovery advocacy, etc.
I am particularly frustrated that so many words are devoted to what others should say, should not say, attacking character, complaining about the other “side”, criticizing others without offering meaningful counterpoints, etc. Too many responses seek to end conversation rather than start or engage others in conversation.
Like any movement, the recovery movement carries many questions that may never really be answered with finality and must be re-asked and re-answered. Those answers may expand or narrow the scope of the movement. For example, we must ask questions like, “who do we exist for?”, “who are we accountable to?”, “who do we represent?”, “what are our values?”, “who needs to be involved to discern the answers to these questions?”, etc.
There was a time when the recovery advocacy movement probably identified as existing for people in recovery and people seeking recovery. It then expanded to people with addiction. Many now see the scope expanding to people who use drugs and people at risk for a drug charge. These matters are important and worthy of discussion.
At any rate, I want to celebrate Phil and Bill for exploring these questions in a way that invites more dialogue and exploration. I hope others continue the conversation.
 We are pleased to announce the release of our newest Tips & Tools for Recovery that Works! video The DISARM Method. In this video we define DISARM, share its history, show how to objectify urges, and what to do when they happen . Checkout the SMART Toolbox for additional resources. Click here to watch this helpful video on our YouTube […]
We are pleased to announce the release of our newest Tips & Tools for Recovery that Works! video The DISARM Method. In this video we define DISARM, share its history, show how to objectify urges, and what to do when they happen . Checkout the SMART Toolbox for additional resources. Click here to watch this helpful video on our YouTube […]
 Growing up, Betty Jacobs knew her family and the community would not be open and accepting of her sexual orientation, so she hid her true identity. She followed the “normal” route and got married and had children because being a mom was something she always wanted. But there was more to Betty that people needed […]
Growing up, Betty Jacobs knew her family and the community would not be open and accepting of her sexual orientation, so she hid her true identity. She followed the “normal” route and got married and had children because being a mom was something she always wanted. But there was more to Betty that people needed […]
Research at the Intersection of HIV with Substance Use Disorders amidst the COVID-19 Pandemic
mfleming
Tue, 07/28/2020 - 16:08
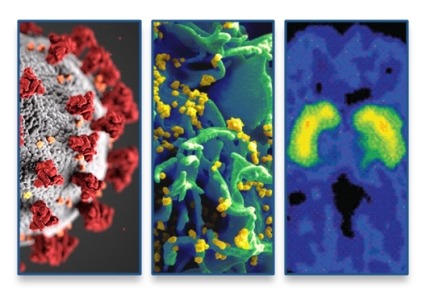
I have written previously about intersections of substance use and substance use disorders (SUDs) with vulnerability to COVID-19 and adverse clinical outcomes. But we also cannot overlook important research on the overlaps of substance use and HIV and AIDS. NIDA and other NIH institutes are using supplementary funds to expand or adapt existing research projects to study the intersection of various health issues with the COVID-19 pandemic. We are prioritizing research into how the coexisting crises of COVID-19, HIV, and substance use, including the opioid crisis, combine to create a disastrous storm, taking lives and overtaxing America’s public health systems.
Research has demonstrated that people with SUDs are at increased risk for acquiring and transmitting HIV, both as a result of sharing injection equipment and because substance use may increase the likelihood of impulsive sex and sex without use of condoms or other HIV prevention tools. For decades, NIDA has devoted considerable resources to support research at the intersection of HIV and substance use. NIDA has the second largest HIV research portfolio at NIH, building unique knowledge related especially to the vulnerable SUD population.
To encourage transformative science and coordinate HIV related research across the institute, NIDA created its AIDS Research Program (ARP) in 2004. In 2008, the ARP established the Avant Garde Awards for HIV/AIDS Research to support individual scientists who propose research relevant to HIV and substance use with high impact potential and that would not typically be funded because of its high risk. In 2015, we launched the Avenir Awards for HIV/AIDS Research to provide grants to early-stage investigators who also propose highly innovative studies.
These commitments to research have led to several significant scientific contributions. A decade ago, NIDA supported a seminal study demonstrating that HIV treatment is prevention, finding that scaling up HIV treatment in people who inject drugs resulted in reductions in community-level viral load and HIV transmission. NIDA-funded research also demonstrated that addiction treatment, especially medications for opioid use disorder, is a necessary part of HIV care and leads to improved viral load, CD4 cell count, and retention in HIV care. A study from NIDA’s Clinical Trials Network found that HIV testing can be integrated into SUD treatment and that counseling offered no additional benefit—findings with broad clinical and public health implications.
The ARP aims also to expand support of basic science research including HIV pathogenesis and the immune response in the presence of addictive substances, including those substances’ ability to promote or interfere with HIV reservoirs in the brain. We are also funding clinical research to develop effective interventions for HIV, substance use, and SUD prevention and treatment, as well as implementation and services research including developing integrated models of care for HIV and SUDs, implementing effective evidence-based practices in routine healthcare settings, and determining the cost and cost-effectiveness of HIV and SUD care. Developing new pre-exposure prophylaxis (PrEP) products to prevent HIV transmission is an ongoing area of research, and NIDA is committed to supporting research to determine feasibility and acceptability of PrEP among people who use drugs.
With additional funds now available to study COVID-19, there is great opportunity for HIV and addiction researchers to make important advances in understanding how COVID-19 intersects with substance use, the opioid epidemic, and HIV. It is already clear that these crises are intertwined and especially impacting vulnerable populations, but many gaps in our understanding remain.
Several co-occurring health problems, including cardiovascular and pulmonary diseases and diabetes, confer greater risk of SARS-CoV-2 infection, severity of disease, and poor outcomes. Additional research could inform us about the clinical impact of COVID-19 on people who use drugs and are living with HIV, as well as the impact that mitigation strategies like social distancing is having on individual health, mental health, and substance use and access to HIV and SUD treatment services. And while knowledge is expanding on how substance use and HIV impact the brain and central nervous system, we know nothing of synergistic short or long-term effects in the presence of COVID-19. There is great potential for knowledge and experience from AIDS care to inform COVID-19 treatment, and conversely, care strategies learned during the COVID-19 crisis could be adapted to HIV outbreaks still seen worldwide that are often connected to injection drug use.
Simply developing effective treatments is no guarantee people using drugs will receive benefit, therefore we cannot expect the development of vaccines or treatments for COVID-19 to confer benefit to this population. When these interventions are available, research will be needed to ensure people using drugs and living with HIV have access. Particularly crucial to study are intersections of HIV, SUD, and COVID-19 among racial and ethnic minority groups, including African Americans, who are consistently disproportionately burdened with poor outcomes across these health conditions. With African Americans suffering and dying from COVID-19 and HIV at higher rates and facing rapidly increasing rates of overdose mortality, research into structural racism and resulting health disparities is more critical than ever. This should include research into stigma within healthcare, which can impede access to care for people of color and those living with HIV and drug addiction.
We cannot forget that in the intense climate of COVID-19, HIV remains a high-priority research area for NIDA. We must develop interventions that are both effective and widely available to address HIV among people who use drugs. The ambitious goal of ending the transmission of HIV will never be realized if we do not also address drug use while ensuring there are no disparities in access to treatment of HIV and SUD.
More information, including funding opportunities, is available through NIDA’s AIDS Research Program.
Comments
Add new comment
Recovery Tip from a Counselor: Utilizing Tools in Long-Term Recovery
Fellowship Hall Counselor, Katherine Barron
This blog is a part of our ongoing series on recovery tips. Each month, a Fellowship Hall counselor will give our readers their very best tips for getting treatment, being successful in therapy and maintaining sobriety. Be sure to read them all.
Katherine Barron’s best tips and advice for long-term recovery.
Often you don’t realize it, but long-term recovery looks a lot like early recovery. Successful early recovery utilizes the same tools that should be used in the long-term. Part of the challenge here is that these tools or methods of supporting our sobriety can seem too simple to us as time goes on. Yes, the tools are incredibly simple, but they are effective. No matter how long you have been sober, using those tools you learned during treatment while working through the steps will always be helpful and reliable.
Something that is crucial to a successful long-term recovery is understanding when you cannot control specific situations in your life–perhaps a conflict in a work or personal relationship of yours. When you’re dealing with something like this, turn back to early steps of acknowledging powerlessness, and turn it over to your higher power, a sponsor, or the collective wisdom of a home group that you feel safe with. This seems simple, but sometimes can be difficult to do. The challenge is that in long-term recovery you may feel like you should already have it “all figured out,” but that’s not the case. There’s more of your own experience that’s available to you, but as life begins to progress and present new conflicts and challenges, you have to utilize your tools and work your program to meet the demands of the day-to-day of your recovery.
When you’re working your 12 step program, helpful habits for successful long-term recovery are:
- Going to meetings
- Talking to a sponsor
- Engaging in the community
- Working steps
- Having a prayer and meditation life
- Addressing what your personal needs are
- Connecting with an outside of the program spiritual life
- Having friends that you connect with and feel supported by inside of the rooms and outside of them.
Engaging in Service
Service is a huge part of long-term recovery. Ask yourself how you can continue to support the entities around you that allowed you to have this healthier and fuller life in recovery. Being in service of other people in the direction of help is really important because it can boost your self-esteem. This is critical because in sobriety the view we have of ourselves has to be addressed, and it is several times throughout the steps.
Humility
The fifth step says about humility, “knowing who and what we really are followed by a sincere attempt to become what we could be,” and that’s honest. That’s saying that you accept yourself where you are–even when it is difficult to do so. Humility is really important because you have to get honest with yourself in long-term recovery. Denial will protect you for a long time because sometimes it is hard to handle all of the “pieces” of yourself. You must have a safe space where you can unpack what has kept you sick and practice that humility. By addressing these things, you can then begin to grow and progress.
Acceptance
We’re living in a challenging time with the current state of the world. Recovery tools are the same but the circumstances are extreme. This is something you should pay attention to, honor and address how it affects you. Acknowledging the reality of what we’re living in right now is important. We’re always powerless but right now it’s so obvious, it’s in our face constantly, and it’s terrifying because naturally as humans we need that illusion of control to feel safe. But the tools are there for you to succeed regardless, and part of your program is accepting that feeling of powerlessness.
Forgiveness & Humor
Long-term recovery also requires a lot of self-forgiveness. That comes up in the steps, but reintroduces itself as meeting yourself where you’re at in the present moment (humility) so that you can make choices based in reality. Also a sense of humor is required–an ability to not take yourself so seriously, an ability to laugh. That sometimes gets lost in active addiction, but is important to long-term recovery.
Katherine, what would you say to someone who may be struggling to stay sober right now?
A day at a time. An hour at a time. I would say that if part of the challenge you’re facing right now is connection, you have to remember it is an action-based program. You have to take action before you feel like it. If you wait until you’re struggling to feel like it’s finally time to do something in the direction of your recovery, then you’re in danger. You have to act your way into right thinking, it doesn’t tend to work the other way around. Remember: feelings are not facts. They’re valid, and they’re important, and they’re pieces of information you need to process your life experiences, but they’re not facts.
I do think that phrase, you’re either walking towards our next use, or away from it is true. Ask yourself, am I engaging in something today that’s helping me walk towards my recovery?
Finally, reach out. You don’t have to feel like it, often you won’t. But do it anyway. You may start to feel very separate and apart but remember, so many around you are having these feelings of anger, and loneliness, and fear, and separation, and if you speak up about it somebody will step up and say me too.
At Fellowship Hall, we’re working to constantly provide support and care both on-campus and digitally those in recovery. For more information, resources, and encouragement, ‘like’ the Fellowship Hall Facebook page and follow us on Instagram at @FellowshipHallNC.
About Fellowship Hall
Fellowship Hall is a 99-bed, private, not-for-profit alcohol and drug treatment center located on 120 tranquil acres in Greensboro, N.C. We provide treatment and evidence-based programs built upon the Twelve-Step model of recovery. We have been accredited by The Joint Commission since 1974 as a specialty hospital and are a member of the National Association of Addiction Treatment Providers. We are committed to providing exceptional, compassionate care to every individual we serve.

“What is past is prologue” as William Shakespeare once said. While this does not mean that history is fated to repeat itself, it does point to the tendency for patterns to echo. Understanding those patterns can help us understand the present and potential risks we face currently. Readers interested in learning about our history, the authoritiave work on the subject is Bill White’s Slaying the Dragon. One of these “echoes” is a tendency to marginalize communities in recovery participating in the development and implementation of the polices and processes related to treatment and recovery from substance use disorders.
There is evidence of erosion in the progress we have made to ensure that people in recovery whose role it is to focus on recovery are at the table when decisions are made about us. Our stories are still valued when they serve other’s needs, but our involvement in matters related to our care perhaps unfortunately less so. This kind of marginalization has occurred historically and so is a concerning trend at this juncture.
An example of marginalization that I observed occurred a few weeks ago for me when I was working with a group and the history of the CRS credential in Pennsylvania came up. The SUD peer credential for the state of Pennsylvania was developed through grassroots efforts by recovery community organizations for use within our communities for persons to engage in and sustain recovery. Our very development of the credential was missing from the body of work being reviewed. Additionally, all reference to recovery community organizations were also absent.
A few weeks later, I was working with another group on a document and a discussion of the definition of a recovery community organization occurred. Some non-recovering participants wanted to remove the word “authentic” from the definition of a recovery community organization. It is a central element of the definition defined by Valentine, White, Taylor in 2007 where the authenticity of voice is highlighted as a critical component.
What does it mean twenty years into the new recovery advocacy movement when we must fight for the very right to define ourselves?
The vast majority of decisions made about persons with addictions are still made with no one in recovery in the room who are focused on the needs of the recovery community. When we are included, it is often in a token role or with persons cherry picked to reflect the desired outcome or share our story to highlight someone else’s agenda. It is by definition paternalistic and exclusionary. History shows us that this tends to move us away from policy (and resources) that serves our community and ultimately away from the very needs of the community. This is a fairly persistent historical pattern.
The opioid crisis and the influence of implicit bias have exacerbated these dynamics. The sad truth of the matter is that while we have made progress in making recovery more visible in society, we have not moved the needle very much on the underling dynamics of marginalization. There remain deep biases against person in recovery which lend themselves to paternalistic processes that do not serve us well. This play out in a variety of ways, including burgeoning administrative demands on our SUD care system and greater disparity in accessing care for an SUD in comparison to medical care and lower compensation for our SUD workforce than social workers or mental health counselors. It is still true here in Pennsylvania and beyond that having a substance use condition is viewed in a more negative light than a mental health condition. Until this changes, there will be a tendency to discount and marginalize our voices.
So what does inclusion look like? According to this 2014 study focused on education there are five essential elements have emerged in looking at inclusion:
- Relationships with the individuals and groups that involve deep connection and awareness of their diverse needs.
- Shared experiences with these groups that bring them into the process in meaningful ways that foster deep insight and empathy for the affected community.
- Advocacy the absence of which not only results in non-participation but the lack of voice. Without an advocate to push for inclusion, and lacking the skills to effectively speak for oneself, a situation of exclusion more readily emerges.
- A sense of identity in which there is sensitivity towards and deliberate focus on fostering a sense of identity and understanding the shared focus of the group in a truly representative manner.
- Transparency, runs through the entire system and involves the seeing of what is present, but also seeing what is not. With an increased awareness of inclusion (and its flip side, exclusion), how values are put into practice in an open, intentional and respectful manner.
Policy that excludes the recovery community moves away from the needs of that very same community; it is the wrong path. Inclusion in deep, meaningful ways strengthen policy and supports recovery across all of our communities. This is what history teaches us. We should be wary of increasing marginalization and paternalism and seek ways to provide meaningful inclusion. Recovery ultimately occurs in the context of community and we cannot effectively support recovery without including the recovery community.
Nothing about us, without us is our historical rallying cry for good reason.
Our community deserves nothing less than full inclusion in matters related to our own care.
Congress Passes Veterans Treatment Court Coordination Act
On July 20, Congress passed the Veterans Treatment Court Coordination Act of 2019 and is expected to be signed into law by President Trump. The act ensures the Department of Justice and its Bureau of Justice Assistance (BJA) continues its outstanding leadership in advancing the veterans treatment court field and makes no changes to the existing veterans treatment court program at BJA.
Since the inception of the veterans treatment court movement, NADCP has led the effort on Capitol Hill to secure federal funding and congressional authorization for the program. As a result, the Veterans Treatment Court Program was congressionally authorized in 2016. In the years since, NADCP and the veterans treatment court field have fought to increase funding. The current $23 million authorization from Congress is a testament to bipartisan support this effort has achieved.
“NADCP is grateful for the strong support Congress has shown for veterans treatment courts,” said NADCP CEO Carson Fox. “Since the first veterans treatment court launched in 2008, it has been our honor to lead this movement.”
For over a decade, BJA has provided funding for communities to start and enhance a veterans treatment court, including supporting NADCP’s Justice For Vets in providing research-driven training and technical assistance. The Veterans Treatment Court Coordination Act demonstrates the widespread congressional support for this program and its importance to the veterans treatment court field.
“The Department of Justice has been an incredible leader in supporting and sustaining veterans treatment courts,” said Justice For Vets Director Scott Tirocchi. “Justice For Vets is honored to assist their critical work by providing comprehensive, research-driven training and technical assistance to the veterans treatment court field.” Together, NADCP and Justice For Vets will continue to meet the needs of veterans treatment courts across the nation.
The post Congress Passes Veterans Treatment Court Coordination Act appeared first on NADCP.org.
The scope of substance use in older adults
While illicit drug use typically declines after young adulthood, nearly 1 million adults aged 65 and older live with a substance use disorder (SUD), as reported in 2018 data.1 While the total number of SUD admissions to treatment facilities between 2000 and 2012 differed slightly, the proportion of admissions of older adults increased from 3.4% to 7.0% during this time.2
Are older adults impacted differently by alcohol and drugs?
Aging could possibly lead to social and physical changes that may increase vulnerability to substance misuse. Little is known about the effects of drugs and alcohol on the aging brain. However, older adults typically metabolize substances more slowly, and their brains can be more sensitive to drugs.3 One study suggests that people addicted to cocaine in their youth may have an accelerated age-related decline in temporal lobe gray matter and a smaller temporal lobe compared to control groups who do not use cocaine. This could make them more vulnerable to adverse consequences of cocaine use as they age.19
Older adults may be more likely to experience mood disorders, lung and heart problems, or memory issues. Drugs can worsen these conditions, exacerbating the negative health consequences of substance use. Additionally, the effects of some drugs—like impaired judgment, coordination, or reaction time—can result in accidents, such as falls and motor vehicle crashes. These sorts of injuries can pose a greater risk to health than in younger adults and coincide with a possible longer recovery time.
Prescription Medicines
Chronic health conditions tend to develop as part of aging, and older adults are often prescribed more medicines than other age groups, leading to a higher rate of exposure to potentially addictive medications. One study of 3,000 adults aged 57-85 showed common mixing of prescription medicines, nonprescription drugs, and dietary supplements. More than 80% of participants used at least one prescription medication daily, with nearly half using more than five medications or supplements,5 putting at least 1 in 25 people in this age group at risk for a major drug-drug interaction.5
Other risks could include accidental misuse of prescription drugs, and possible worsening of existing mental health issues. For example, a 2019 study of patients over the age of 50 noted that more than 25% who misuse prescription opioids or benzodiazepines expressed suicidal ideation, compared to 2% who do not use them, underscoring the need for careful screening before prescribing these medications.6
Opioid Pain Medicines
Persistent pain may be more complicated in older adults experiencing other health conditions. Up to 80% of patients with advanced cancer report pain, as well as 77% of heart disease patients, and up to 40% of outpatients 65 and older.8 Between 4-9% of adults age 65 or older use prescription opioid medications for pain relief.7 From 1995 to 2010, opioids prescribed for older adults during regular office visits increased by a factor of nine.7
The U.S. population of adults 55 and older increased by about 6% between 2013-2015, yet the proportion of people in that age group seeking treatment for opioid use disorder increased nearly 54%.4 The proportion of older adults using heroin—an illicit opioid—more than doubled between 2013-2015,4 in part because some people misusing prescription opioids switch to this cheaper drug.4
Marijuana
Nine percent of adults aged 50-64 reported past year marijuana use in 2015-2016, compared to 7.1% in 2012-2013.10 The use of cannabis in the past year by adults 65 years and older increased sharply from 0.4% in 2006 and 2007 to 2.9% in 2015 and 2016.22
Medical Marijuana
One U.S. study suggests that close to a quarter of marijuana users age 65 or older report that a doctor had recommended marijuana in the past year.10 Research suggests medical marijuana may relieve symptoms related to chronic pain, sleep hygiene, malnutrition, depression, or to help with side effects from cancer treatment.11 It is important to note that the marijuana plant has not been approved by the Food and Drug Administration (FDA) as a medicine. Therefore, the potential benefits of medical marijuana must be weighed against its risks, particularly for individuals who have other health conditions or take prescribed medications.11
Risks of Marijuana Use
Regular marijuana use for medical or other reasons at any age has been linked to chronic respiratory conditions, depression, impaired memory, adverse cardiovascular functions, and altered judgement and motor skills.12 Marijuana can interact with a number of prescription drugs and complicate already existing health issues and common physiological changes in older adults.
Nicotine
The Centers for Disease Control and Prevention (CDC) reports that in 2017, about 8 of every 100 adults aged 65 and older smoked cigarettes, increasing their risk for heart disease and cancer.20 While this rate is lower than that for younger adults, research suggests that older people who smoke have increased risk of becoming frail, though smokers who have quit do not appear to be at higher risk.14 Although about 300,000 smoking-related deaths occur each year among people who are age 65 and older, the risk diminishes in older adults who quit smoking.13 A typical smoker who quits after age 65 could add two to three years to their life expectancy. Within a year of quitting, most former smokers reduce their risk of coronary heart disease by half.13
Nicotine Vaping
There has been little research on the effects of vaping nicotine (e-cigarettes) among older adults; however, certain risks exist in all age groups. Some research suggests that e-cigarettes might be less harmful than cigarettes when people who regularly smoke switch to vaping as a complete replacement. However, research on this is mixed, and the FDA has not approved e-cigarettes as a smoking cessation aid. There is also evidence that many people continue to use both delivery systems to inhale nicotine, which is a highly addictive drug.
Alcohol
Alcohol is the most used drug among older adults, with about 65% of people 65 and older reporting high-risk drinking, defined as exceeding daily guidelines at least weekly in the past year.16 Of particular concern, more than a tenth of adults age 65 and older currently binge drink,18 which is defined as drinking five or more drinks on the same occasion for men, and four or more drinks on the same occasion for women. In addition, research published in 2020 shows that increases in alcohol consumption in recent years have been greater for people aged 50 and older relative to younger age‐groups.21
Risk Factors for Substance Use Disorders in Older Adults
Physical risk factors for substance use disorders in older adults can include: chronic pain; physical disabilities or reduced mobility; transitions in living or care situations; loss of loved ones; forced retirement or change in income; poor health status; chronic illness; and taking a lot of medicines and supplements. Psychiatric risk factors include: avoidance coping style; history of substance use disorders; previous or current mental illness; and feeling socially isolated.19
Alcohol Use Disorder: Most admissions to substance use treatment centers in this age group relate to alcohol.2 One study documented a 107% increase in alcohol use disorder among adults aged 65 years and older from 2001 to 2013.16 Alcohol use disorder can put older people at greater risk for a range of health problems, including diabetes, high blood pressure, congestive heart failure, liver and bone problems, memory issues and mood disorders.16
How are substance use disorders treated in older adults?
Many behavioral therapies and medications have been successful in treating substance use disorders in older adults.
Little is known about the best models of care, but research shows that older patients have better results with longer durations of care.7 Ideal models include diagnosis and management of other chronic conditions, re-building support networks, improving access to medical services, improved case management, and staff training in evidence-based strategies for this age group.7
Providers may confuse SUD symptoms with those of other chronic health conditions or with natural, age-related changes. Research is needed to develop targeted SUD screening methods for older adults. Integrated models of care for those with coexisting medical and psychiatric conditions are also needed.2 It is important to note that once in treatment, people can respond well to care.2
Read more about drug addiction treatment in our Treatment Approaches for Drug Addiction DrugFacts.
Points to Remember
- While use of illicit drugs in older adults is much lower than among other adults, it is currently increasing.
- Older adults are often more susceptible to the effects of drugs, because as the body ages, it often cannot absorb and break down drugs and alcohol as easily as it once did.
- Older adults are more likely to unintentionally misuse medicines by forgetting to take their medicine, taking it too often, or taking the wrong amount.
- Some older adults may take substances to cope with big life changes such as retirement, grief and loss, declining health, or a change in living situation.
- Most admissions to substance use treatment centers in this age group are for alcohol.
- Many behavioral therapies and medications have been successful in treating substance use disorders, although medications are underutilized.
- It is never too late to quit using substances—quitting can improve quality of life and future health.
- More science is needed on the effects of substance use on the aging brain, as well as into effective models of care for older adults with substance use disorders.
- Providers may confuse symptoms of substance use with other symptoms of aging, which could include chronic health conditions or reactions to stressful, life-changing events.
Additional Resources
Learn More
For more information about substance use in older adults, visit:
References
- Substance Abuse and Mental Health Services Administration. (2019). Results from the 2018 National Survey on Drug Use and Health: Detailed tables. Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. Retrieved from https://www.samhsa.gov/data/
- Chatre S, Cook R, Mallik E et al. Trends in substance use admissions among older adults. BMC Health Services Research. 2017; 584(17). doi: https://doi.org/10.1186/s12913-017-2538-z
- Colliver JD, Compton WM, Gfroerer JC, Condon T. Projecting drug use among aging baby boomers in 2020. Annals of Epidemiology. 2006; 16(4): 257–265.
- Huhn AS, Strain EC, Tompkins DA, Dunn KE. A hidden aspect of the U.S. opioid crisis: Rise in first-time treatment admissions for older adults with opioid use disorder. Drug Alcohol Depend. 2018 Dec 1; 193: 142-147. doi: 10.1016/j.drugalcdep.2018
- Qato DM, Alexander GC, Conti RM, Johnson M, Schumm P, Lindau ST. Use of prescription and over-the-counter medications and dietary supplements among older adults in the United States. JAMA. 2008 Dec 24; 300(24): 2867-2878. doi: 10.1001/jama.2008.892
- Schepis TS, Simoni-Wastila L, McCabe SE. Prescription opioid and benzodiazepine misuse is associated with suicidal ideation in older adults. Int J Geriatr Psychiatry. 2019; 34(1): 122-129. doi: 10.1002/gps.4999
- Lehmann S, Fingerhood M. Substance-use disorders in later life, N Engl J Med. 2018 December 13; 379(24): 2351-2360. doi: 10.1056/NEJMra1805981
- Galicia-Castillo, M. Opioids for persistent pain in older adults. Cleveland Clinic Journal of Medicine. 2016 June 6; 83(6). Retrieved from: https://mdedge-files-live.s3.us-east-2.amazonaws.com/files/s3fs-public/issues/articles/Galicia-Castillo_OpiodsForOlderAdults.pdf
- Wu LT, Blazer DG. Illicit and nonmedical drug use among older adults: A review. Journal of Aging and Health. 2011; 23(3): 481–504. doi:10.1177/0898264310386224
- Han BH, Palamar JJ. Marijuana use by middle-aged and older adults in the United States, 2015-2016. Drug Alcohol Depend. 2018; 191: 374-381. Retrieved from: https://www.ncbi.nlm.nih.gov/pubmed/30197051
- Abuhasira R, Ron A, Sikorin I, Noack V. Medical cannabis for older patients—Treatment protocol and initial results. Journal of Clinical Medicine. 2019; 8(11): 1819. https://doi.org/10.3390/jcm8111819
- Volkow N, Baler R, Compton W, Weiss S. Adverse health effects of marijuana use. N Engl J Med. 2014 June 5; 370(23): 2219-2227. doi: 10.1056/NEJMra1402309
- Centers for Disease Control and Prevention. Smoking and Older Adults. November 2008. https://www2c.cdc.gov/podcasts/media/pdf/HealthyAgingSmoking.pdf. Accessed March 12, 2020.
- Kojima G, Iliffe S, Jivraj S, Liljas A, Walters K. Does current smoking predict future frailty? The English longitudinal study of ageing. Age and Ageing. 2018 January; 47(1): 126-131. https://doi.org/10.1093/ageing/afx136
- Older adults fact sheet. National Institute on Alcohol Abuse and Alcoholism. https://www.niaaa.nih.gov/alcohol-health/special-populations-co-occurring-disorders/older-adults
- Grant BF, Chou SP, Saha TD, et al. Prevalence of 12‐month alcohol use, high‐risk drinking, and DSM‐IV alcohol use disorder in the United States, 2001‐2002 to 2012‐2013: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. JAMA Psychiat. 2017; 74(9): 911‐923.
- Kuerbis et al. Substance abuse among older adults. Clin Geriatr Med. 2014 Aug; 30(3): 629–654. doi:10.1016/j.cger.2014.04.008
- Han B, Moore A, Ferris R, Palamar J. Binge drinking among older adults in the United States, 2015-2017. Journal of the American Geriatrics Society. 2019 July 31; 67(10). https://doi.org/10.1111/jgs.16071
- Bartzokis et al. Magnetic resonance imaging evidence of “silent” cerebrovascular toxicity in cocaine dependence. Biol Psychiatry. 1999; 45: 1203-1211.
- Current cigarette smoking among adults in the United States fact sheet. Centers for Disease Control and Prevention. https://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/index.htm
- White A, Castle I, Hingson R, Powell P. Using death certificates to explore changes in alcohol‐related mortality in the United States, 1999 to 2017. Alcoholism Clinical and Experimental Research. 2020 January 7; 44(1): 178-187. https://doi.org/10.1111/acer.14239
- Han BH, Sherman S, Mauro PM, Martins SS, Rotenberg J, Palamar JJ. Demographic trends among older cannabis users in the United States, 2006-2013. Addiction. 2017; 112(3): 516-525. doi:10.1111/add.13670
This publication is available for your use and may be reproduced in its entirety without permission from NIDA. Citation of the source is appreciated, using the following language: Source: National Institute on Drug Abuse; National Institutes of Health; U.S. Department of Health and Human Services.
Is the person that is speaking relatively known or relatively unknown to us?
- Do we hear their words, or do we hear them (their person)?
- As we listen, how do we determine if we hear or neglect their words?
- As we listen, how do we determine if we hear or neglect their person?
As we listen, do we apprehend the transcendent?
- Do their words obscure their person from us? Or do we hear their person?
- To the extent we know them, are either their words or person obscured by our knowledge of them?
- To the extent we know them, do we hear our projections instead of them and their words?
Is our history (personal or professional) in the way of hearing?
- Do we hear with quality?
- Do we hear with coherence?
- Are we hearing the person’s desired outcome instead of hearing their person?
- Does our desired outcome for them obscure us from hearing their words? Or from hearing their person?
- What theory, tradition, or discipline of theirs is in their way?
- What theory, tradition, or discipline of ours is in our way?
- Are we employing an objective arrangement instead of listening?
- Are we hearing, or only following a narrative of words?
What is being said?
What is the person saying?
Inspired by a fresh reading of:
Foucault, M. (1969). What Is An Author? Lecture given at the Collège de France.
Dear Diary…How Journaling as an Adult can Benefit Long-Term Recovery

When you hear the word journaling what comes to mind? For most, the idea of journaling invokes images of our younger selves writing about things that seem trivial now–the birthday party you weren’t invited to, or a carnation at school from your Valentine. You may even remember an occasional entry you wrote while you were away at a summer camp. How do you think journaling could fit into your adult life? Your life during your recovery?
Journaling is an incredibly powerful tool for reflection, introspection, and growth as you progress in your sobriety. It’s not just an asset or a helpful tool–it is an essential component of your recovery for long-term success.
The benefits of Journaling in Recovery
It’s free, and you can do it anytime, anywhere.
You can bring your journal and pen with you to work, to school, to the park, etc. You can journal during your commute (if you’re not driving) or on your breaks at work–you can journal anywhere that is comfortable for you. Best of all? It is a completely free (aside from your pen and paper costs) therapeutic act.
Putting pen to paper can help make sense of what you’re thinking and feeling.
Oftentimes when you experience intense waves of thoughts, they can be messy, sporadic, scattered, overwhelming, and hard to make sense of. By journaling, you are able to take control of your feelings and thoughts, instead of allowing them to control you.
You can tap into things you may not have been able to clearly access just through thinking.
In the same way that you may converse with a counselor or a sponsor, journaling allows you to “talk” or rather, write, through situations, thoughts, and emotions. Further, journaling provides an avenue to dig deep and intimately interact with the self. Knowing that there is no judgement, no revealing nature to it, and that you are only writing for yourself can provide you with a sense of true security that allows you to be even more honest and open than you may have been with another party involved.
Writing your thoughts down makes them real.
 Emotions experienced during your recovery are unique in that without substances, you are essentially re-learning how to process and fully feel again. The act of writing these feelings down benefits you in several ways; you’re able to actualize and validate what you are or have been feeling and experiencing. From this, you’re able to separate yourself from any fleeting or less permanent feelings and put space between your thoughts and actions. This is a huge benefit that can be used as a tool to prevent you from making permanent decisions based on more temporary feelings. For example, when you have a craving or notice a trigger, digging deep into those feelings, making them real, and making peace with them can be invaluable in preventing relapse or slip-ups. In doing this, you’re also able to return to these entries or times when you have succeeded in overcoming temptation and use them as inspiration on harder days.
Emotions experienced during your recovery are unique in that without substances, you are essentially re-learning how to process and fully feel again. The act of writing these feelings down benefits you in several ways; you’re able to actualize and validate what you are or have been feeling and experiencing. From this, you’re able to separate yourself from any fleeting or less permanent feelings and put space between your thoughts and actions. This is a huge benefit that can be used as a tool to prevent you from making permanent decisions based on more temporary feelings. For example, when you have a craving or notice a trigger, digging deep into those feelings, making them real, and making peace with them can be invaluable in preventing relapse or slip-ups. In doing this, you’re also able to return to these entries or times when you have succeeded in overcoming temptation and use them as inspiration on harder days.
Reflection is necessary
In steps 4 and 10 we are asked to take inventory of ourselves, our experiences, our past, how this has all affected us, and in turn, how this has caused us to affect others.
Step 4 (AA/NA) Made a searching and fearless moral inventory of ourselves.
Step 10 (AA/NA) Continued to take personal inventory and when we were wrong promptly admitted it.
The thoughtfulness and consideration required for these steps translates beautifully into journaling. Journaling allows us to clear the wreckage of our past and gain true understanding in regard to how we can move forward in our life and recovery.
Get into a routine.
Step 10 asks that we continue to take inventory of our days. This is why it is important to get into a routine of journaling consistently. In your recovery, your tools can only help you if you make a true commitment to them and consistently utilize them. Set a reminder in your phone and dedicate yourself to some sort of journaling, if only for a few minutes a day.
Some journaling styles to consider for beginners:
Bullet Journaling- Kept in the style of a list. This is a great way to begin journaling, as you can take inventory or make simple lists of your day to day actions, thoughts, and feelings.
Gratitude Journal– In contrast to other styles of journaling, a gratitude journal focuses on the areas of your life for which you are thankful. The school of thought that inspires this style of journaling believes that we should call attention to the positive things in our days rather than giving any energy to the negative aspects. Through gratitude journaling, you can review passages and remind yourself of all you have to be thankful for.
Free write journaling– This is also a great style of journaling for you if you’re just getting into the habit of writing. Put on some of your favorite relaxing music, and set a timer on your phone for 10 minutes. For the full 10 minutes write whatever comes to your head. Don’t think twice about it—write exactly what you think and feel. After the 10 minutes are up, review what you’ve written and reflect on how this passage makes you feel. This is a great way to separate yourself from temporary emotions.
The act of daily journaling can be beneficial for everyone, but especially for you during your recovery. Find a routine and a style of journaling that works for you, and dedicate yourself to consistently utilizing this new tool. For more helpful tools and resources be sure to follow us on Facebook, Instagram and LinkedIn at @FellowshipHallNC
About Fellowship Hall
Fellowship Hall is a 99-bed, private, not-for-profit alcohol and drug treatment center located on 120 tranquil acres in Greensboro, N.C. We provide treatment and evidence-based programs built upon the Twelve-Step model of recovery. We have been accredited by The Joint Commission since 1974 as a specialty hospital and are a member of the National Association of Addiction Treatment Providers. We are committed to providing exceptional, compassionate care to every individual we serve.
NIDA Research
on August 3, 2020
I have been in this field for over 50 years. The investment the taxpayer has made in NIDA research is quite disappointing to me. Prevention - the drug abuse problem is worse than ever and the strategies for prevention have not been successful, Treatment - the only curriculum supported by NIDA is the Matrix, we do have evidence-based treatment, not sure NIDA has had much to do with it. MAT - the sole focus on opiates and the lack of recognition of methamphetamine as the primary drug of choice and problem in the western part of the country and on the reservations is a big hole that NIDA should have focused on and now we are in no-man's land. Great disappointment. In fact, the focus on HIV, MAT and Opiates has been a big disappointment (what MAT drugs work best with which opiate clients - who should be on MAT and who doesn't need it) while other areas like prevention, methamphetamine MAT and related treatment, Native American treatment effectiveness, and effective recovery strategies have been sorely neglected. The direction of management at NIDA for the research dollar is very questionable. The gains made for all the money spent on biological research is minimal.
Just my thoughts.