

C.C.’s passion and enthusiasm towards his recovery is infectious. He uses the SMART Recovery tools and resources to cope with urges and manage his addiction. C.C. is happy to share his journey with others, in order to help them live Life Beyond Addiction.
Subscribe to the SMART Recovery YouTube Channel
Video storytelling is a powerful tool in recovery, and we are proud to share our SMART Recovery content free-of-charge, available anywhere, on any device. Our videos hope to inform, entertain, and inspire anyone in the recovery community.
Subscribe to our YouTube channel and be notified every time we release a new video.
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @ 800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!
The question of how to describe and categorize addiction has been the subject of several of my recent posts. Some people scratch their heads about why I care so much about whether we think of it as a disease. Bill White summarized the stakes well here:
If AOD problems could be solved by physically unraveling the person-drug relationship, only physicians and nurses trained in the mechanics of detoxification would be needed to address these problems. If AOD problems were simply a symptom of untreated psychiatric illness, more psychiatrists, not addiction counselors would be needed. If these problems were only a reflection of grief, trauma, family disturbance, economic distress, or cultural oppression, we would need psychologists, social workers, vocational counselors, and social activists rather than addiction counselors. Historically, other professions conveyed to the addict that other problems were the source of addiction and their resolution was the pathway to recovery. Addiction counseling was built on the failure of this premise.
White, W. (2004). The historical essence of addiction counseling. Counselor, 5(3), 43-48.
Whether we define alcoholism as a sin, a crime, a disease, a social problem, or a product of economic deprivation determines whether this society assigns that problem to the care of the priest, police officer, doctor, addiction counselor, social worker, urban planner, or community activist. The model chosen will determine the fate of untold numbers of alcoholics and addicts and untold numbers of social institutions and professional careers.
The existence of a “treatment industry” and its “ownership” of the problem of addiction should not be taken for granted. Sweeping shifts in values and changes in the alignment of major social institutions might pass ownership of this problem to another group.
White, W. L. (1998). Slaying the Dragon: The History of Addiction Treatment and Recovery in America, page 338
I’ll acknowledge that hustles like patient brokering, cash MAT clinics, drug screen scams, and over-priced residential with little continuing care make it difficult to root for the survival of the “treatment industry” but White’s words capture the risks of transferring responsibility to other groups.
What’s made addiction counseling unique has been the emphasis on recovery as the endpoint. More specifically, a model of recovery that results in people with addiction becoming “better than well.”
An essential step in transferring responsibility from one group to another is redefining the problem.
Some efforts to define addiction as something other than a disease argue that it’s not a disease but, more often, arguments against the disease model are more about achieving particular goals (protecting liberties, assigning personal responsibility, advancing particular drug policy goals, advancing social justice, emphasizing particular interventions, stigma reduction, etc.) rather than really questioning whether it’s actually a disease.
Recently, the American Journal of Public Health published an article titled The Harms of Constructing Addiction as a Chronic, Relapsing Brain Disease. I appreciated the clarity of its arguments.
The article opens with the following paragraph:
As an international network of historians and social scientists who study approaches to the management of drugs across time and place, we have noticed the effort to redefine addiction as a chronic, relapsing brain disease (CRBD). The CRBD model is promoted as a route to destigmatize addiction and to empower individuals to access treatment that works within that model’s terms.1 CRBD usefully recognizes that brain-based neural adaptations place individual brains in chronic states of readiness to relapse. But brains are housed inside of people. Substance use is biological, social, and political; our concepts and approaches to complex questions surrounding substance use must be, too.2,3 By overlooking the sociopolitical dynamics and inequalities bound up with substance use, the CRBD model can paradoxically further marginalize people who use drugs by positing them as neurobiologically incapable of agency or choice. We are concerned that the CRBD model paints drug users as individuals whose exclusion from social, economic, and political participation is justified by their biological flaws and damaged brains.
Note that the authors respond to an argument for what the disease model can accomplish — it “is promoted as a route to destigmatize addiction and to empower individuals to access treatment” — rather than to the argument that it is properly classified as a disease.
All illnesses occur within people and have biological, social, and political contexts. Over the past couple of years have reinforced that those contexts have important implications, even with something like a respiratory illness caused by a virus. That COVID is associated with social, economic, and political disruption, conflict, and suffering shouldn’t and wouldn’t lead us to questions about whether COVID is properly framed as a disease.
Choosing between the CRBD model and addressing the sociopolitical dynamics and inequalities seems like a false choice. Why does it have to be either/or? Cant it, shouldn’t it, be both/and?
No responsible advocate of the chronic relapsing brain disease (CRBD) model would argue that people with addiction are incapable of agency or choice. Addiction is a disorder involving choice, but it is typically characterized as impaired choice or intermittent loss of choice, rather than a complete or consistent loss of choice. One might compare this to serious mental illness with intermittent fluctuations in impairment. These fluctuations in impairment may range from no impairment to severe impairment, depending on the individual and the current state of their illness.
It’s also important to note the authors’ switch from discussing the CRBD model in the context of people with addiction to people who use substances. The CRBD model should never be applied to people without addiction.
The article proceeds with a brief examination and critique of the CRBD model. The authors note that advocates of the CRBD model voiced hope that the model would produce a sharp break from the moral models that had dominated responses to addiction.
The supposedly new CRBD model recycles disease concepts that have mixed medical and moral concerns since the 18th century.9 Disease models have been used to support a range of policy approaches from strict prohibition, to compulsory treatment or “civil commitment,” to medical maintenance, to incarceration. In them, addiction has been both criminalized and medicalized; addicts were labeled as sick individuals yet also punished for bad behavior as deviants….
Despite the hopes placed on the new CRBD model, this heritage has not been erased by redefining addiction as a chronic disease located in the brain.11 On the contrary, the brutal social inequalities of US responses to drug-related harms have persisted or even worsened.
Note that this is not actually criticism of the CRBD. Rather, it’s criticism of the fact that the CRBD has not delivered the change in policy and attitudes that many people hoped for.
Framing Addiction as a Chronic, Relapsing Brain Disease
It continues with the suggestion that the CRBD may have accelerated these harms in ways that include criminalization, incarceration, and a molecular orientation that opened the door for the opioid crisis with the false belief that Oxycontin’s extended-release formulation might make it safer.
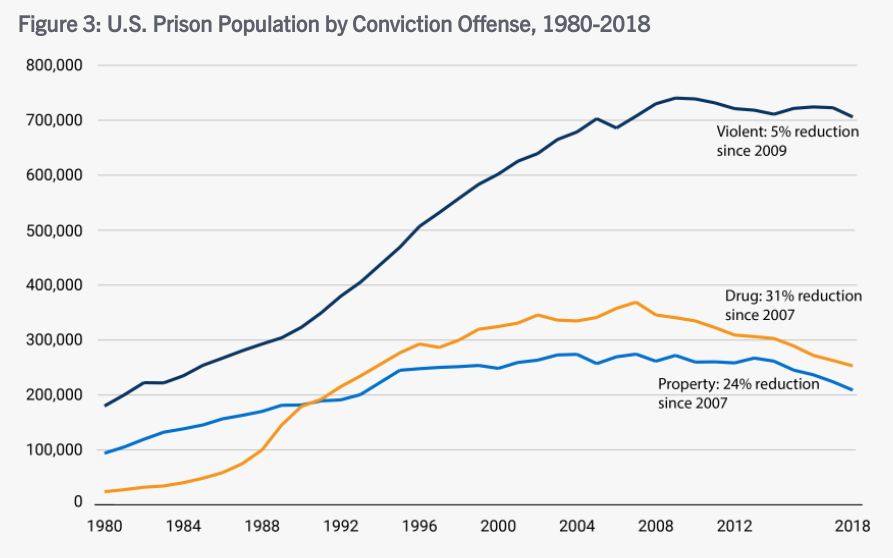
I’m not a believer that the CRBD necessarily leads to less stigma and better policy, and I won’t suggest that the CRBD is responsible for any changes in policy. However, the argument that the CRBD model is associated with incarceration is undermined by trends in incarceration for drug crimes. Even if the CRBD model could deliver significant policy and cultural change, that would take time — years, probably many years. The chart below shows a leveling off and eventual decline of people incarcerated for drug crimes during the period discussed. It’s still too many people incarcerated and those people are disproportionately African American but, if we want to assert an association between the CRBD and incarceration rates, the association would be a downward trend in drug crime incarcerations.
-

A liver cure containing 90% alcohol. -
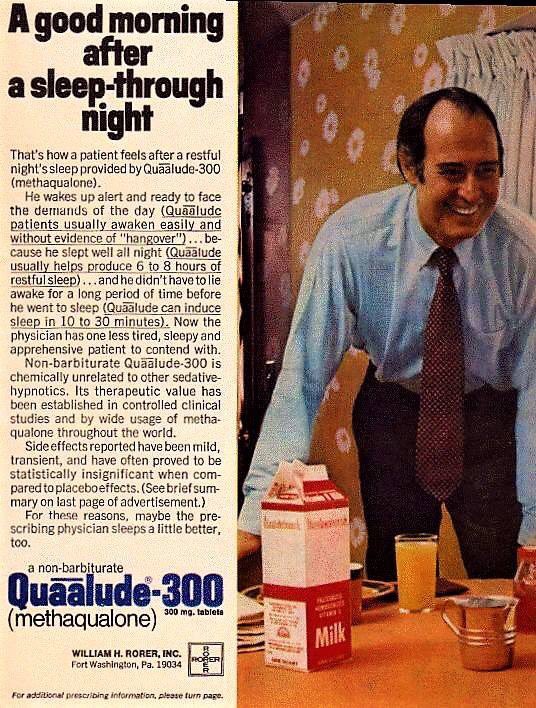
“mild… statistically insignificant side effects”
The Oxycontin argument would be a lot stronger if there wasn’t a long history of pharmaceutical advertising that misrepresented the safety profile of medications, often misrepresenting science to obscure the risks.
So… the criticism is not about the scientific or medical truth of the model, rather it’s about insufficient political and social progress.
This section ends with a strong point:
Expanding access to addiction medications without inclusive social policies and harm reduction has not been enough to prevent or stem America’s opioid crisis.
Calling something a brain disease does not and should not narrow our attention to pills and procedures. Behavioral, psychological, and social interventions ought to be particularly important with a brain disease, particularly since a brain disease is likely to affect those domains and those domains are largely experienced in the brain.
Alternate Frame: Harm Reduction and Social Justice
The authors offer harm reduction and social justice as an alternative frame:
There are other ways of framing and responding to substance use. The most promising of these is harm reduction, a 50-year-old social movement mounted against repressive drug policies. Rather than centering on the brain and embracing abstinence as a goal, harm reduction prioritizes the health and social inclusion of people who use drugs.
Note that the authors are not really speaking to causes or treatments and there’s no reason the recognition of a condition as a disease should omit social inclusion. For example, serious mental illnesses are recognized as diseases and social inclusion should be considered an essential element of effective treatment and policy.
So, what is the concern?
Consumers resist the coercive and often punitive ways in which medications for addiction have been deployed. Harm reduction links the biological to the social without prioritizing one over the other.
So, a concern is coercion. Calling something a brain disease does not necessitate coercion (think Parkinson’s), but it can open the door. In the medical world, that door might be opened through the legal designation of a guardian. With mental illness, involuntary treatment may be sought for patients that pose a risk to themselves or others. In the cases of guardianship and court-ordered treatment for a mental health crisis, there are processes designed to protect the rights of the individual, including time limitations on any court order resulting from the process.
In the case of addiction, involvement with the criminal justice system often leads to coerced treatment. And, there has been far too little systemic ambivalence about individual rights when it comes to coerced treatment (and incarceration) for addiction. Importantly, there’s also been too little concern about systemic injustices, like the disproportionate numbers of African Americans charged and convicted of drug crimes.
Addiction is also unusual among diseases in an important way. As Keith Humphreys pointed out, “To use a term from economics, addictions have high negative externalities that most medical disorders simply do not, and that changes how perfectly decent and reasonable people respond to them.”
To illuminate those high negative externalities, Humphreys poses the following questions:
If you had a financial manager who would have access to all your accounts and personal information, would you consider that person developing a heroin addiction of any more consequence than him/her developing type 2 diabetes? If you were enrolling your child in a preschool, would you react in the same way if informed that the teacher was prone to methamphetamine binges as you would to learning that the teacher was prone to asthma attacks? If asked by a non-expert from outside our field, how would you explain why millions of people have chosen to attend self-help groups and treatment programs focused on recovering from having had an ‘‘alcoholic’’ parent, but there is no demand for recovery programs focused on adult children of hypertensive patients?
Acknowledging that there has been insufficient concern for individual rights, I suppose at least 4 considerations are important regarding coerced treatment.
- Do the circumstances merit limiting the liberties of the person (through court supervision, incarceration, or coerced treatment)? Is this a circumstance where others were harmed or at serious risk of harm? If we removed the substance from the situation, would this still be a matter for the criminal justice (or child protection) system?
- Treatment for what? What is the person’s substance use problem and is the treatment appropriate for that problem? Are we talking about someone with a mild, moderate, or severe problem? Are we talking about someone with a pattern of impaired control?
- Coerced treatment is often an alternative to incarceration. This is a good thing. However, we should be mindful that this option doesn’t lower the bar for limiting the rights of a person.
- What systemic factors are likely to influence who ends up in this system and how their case is handled? Are we acknowledging and addressing those? If forces external to this system are a problem, how can that be mitigated within this system?
I’m ambivalent about the development of processes for addiction that would mirror the mental health processes. Having worked in both systems, I know it would require a lot of work to protect the rights of people with addiction and an enormous amount of work to develop systems of care that can meet the need effectively.
As for the role of the CRBD model in this area, I do see the risk and I do sometimes hear the CRBD model deployed to defend coerced treatment. At the same time, the period of time the authors point to has been characterized by efforts to reduce incarceration and offer treatment as an alternative — on the grounds that addiction is an illness.
I think the CRBD model offers a valuable test for public policy — parity. Would we, should we, treat a cardiac or diabetes patient this way? The high negative externalities identified by Humpreys do present a challenge for parity tests using other chronic diseases, but he offers another frame. He’s talking about it in the context of public education, but it’s relevant for thinking about policy as well.
A better analogy than asthma, type II diabetes, and hypertension we could employ for addiction might be to liken it to chronic infectious illnesses (eg, HIV/AIDS). We accept that for infectious illnesses, some fear of people who have the disease is rational; indeed health professionals exhort people to engage in behavior designed to protect themselves from infected individuals (eg, insisting that a sexual partner with a sexually transmitted disease wear a condom, not personally cleaning the body of someone who died from Ebola). Further, we accept that there is a legitimate role for law enforcement— Typhoid Mary was prevented from continuing to infect people by police (Marinelli et al., 2013), not doctors. Analogizing addictions to infectious diseases has all the virtues of analogizing it to diseases with low externalities (eg, asthma) and also has the unique advantage of better matching the public’s experience of the disorder (and it is them and not ourselves whom we need to persuade).
Of course, this imagery will evoke strong negative reactions from many, but it also provides the potential to narrow the focus for coercive interventions to those where there is actual harm or serious risk to others.
Uneven Progress: Harm Reduction in Europe
Next, the authors provide a little background on harm reduction in Europe that they summarize as follows:
Harm reduction initiatives across Europe and the United Kingdom were introduced as part of publicly funded institutions that often coexist with repressive drug policy systems—something shown with unusual starkness in the French example. The UK example indicates how harm reduction measures do not always center on social justice for people who use drugs but are instead introduced to protect the majority population. The Norwegian example points toward how restrictive access to harm reduction services can facilitate paternalism and reduce agency of people who use drugs.
Conclusion: Human Rights as an Expanded Harm Reduction Frame
…The human rights frame counters some of the CRBD model’s limitations, including the centering on brain disease pathology and insistence on judging each individual as either a patient or a criminal.
People who use drugs are themselves developing community-based harm reduction approaches that resist both criminalization and medicalization on the ground that both have been used to control drug users. Harm reduction critiques hierarchical forms of clinical and neuroscientific expertise and instead supports people who use drugs in recognizing their expertise in managing their own practices and bodies, supporting their agency, and widening their options. Abstinence can be considered part of this approach, but only if chosen by people who use drugs themselves.31 When abstinence is imposed by external forces (medical practitioners, family, law enforcement, or other stakeholders), abstinence itself becomes a risk for overdose death.
This illuminates another objection, that the disease label situates the person with addiction as a patient. (As opposed to a criminal.) It’s also important to note that the authors switched from addiction to “people who use drugs.” This switch is important because using drugs isn’t a disease but may be a symptom of the disease of addiction, just as coughing isn’t tuberculosis. To be sure, most people who use drugs do not have the disease of addiction. Differentiating between people with addiction and other people who use drugs is critically important in many ways, but particularly important when discussing the disease model, its conceptual boundaries, and its utility.
The framework of disease is helpful because it helps us draw a boundary to determine who has the disease and who does not, it can help us understand some of the processes involved and their consequences, it can help us identify treatments, and help us identify treatments, behaviors, and interventions that are contraindicated.
The authors seem to be very focused on protecting the right to choose to use drugs. For the minority of users with addiction, a critical element to understand is impaired control, meaning that drug use is not always freely chosen. (One might even say that, at times, the illness coerces the sufferer to use drugs. This is part of what’s so excruciating for people with addiction and their loved ones.) This is one of the reasons that, for this most severe form of drug problems affecting a minority of users, abstinence is indicated.
People with bipolar or schizophrenia have the right to refuse treatment in most circumstances. However, when their illness results in high negative externalities, they may be coerced into treatment via a process that includes several safeguards to protect their liberties.
So… this critique never seems to make a case that addiction is not a disease. Rather, it argues that the CRBD model has not delivered the change some people promised and they proposed a model centered on the social and political change. I don’t see where an emphasis on social justice requires the abandonment of the disease model. In fact, where high negative externalities are present, the disease model becomes a mitigating consideration, resulting in more just social responses.
I believe it’s true that addiction is a disease and the authors never really made an argument that it isn’t. Should that truth be sacrificed or obscured in pursuit of justice? I don’t think it’s a good idea. It’s the kind of thing that contributes to the current epistemic crisis and it isn’t necessary. Any model can be harmful if it’s misused or implemented in a reductive way that results in the neglect of important considerations. The CRBD is no different.

An interesting discussion with a passionate advocate for MAT expansion and the most prominent advocate for the “new paradigm“:
What is the process for successfully integrating these 2 approaches? What are the biggest hurdles providers face when accomplishing this goal?
Dr DuPont: The biggest hurdle is the staff reluctance, even the staff distaste, for the integration of an alternative as an option for patients who want it. There is an ideological and visceral rejection of the integration at the start that is challenging. But with gentle persistence, it has been overcome and the patients have benefited.
Dr Poland: I also find that patients are a bit reluctant to share their experiences with 12-Step—good or bad—somehow, they’re expecting a reaction from me—either insistence they go or disdain for the program. Again, being open and nonjudgmental about what works for an individual allows us to best care for them. And, I’ve definitely learned a lot from my patients about how to integrate the 2 modalities in a way that complements each other.
I’m looking for a recording.
As substance-free definitions of recovery are challenged, this article on Stanford’s substance-free student housing community made me wonder if some recovering students will find more safety and support, and have more in common with fellow students in these communities than in collegiate recovery programs (CRP) that include students whose definition of recovery includes ongoing substance use.
Maybe this kind of housing option gives a CRP more space to stretch their boundaries, knowing that there is a substance-free peer group elsewhere on campus? Maybe it offers a path to support these students and sidestep culture wars about the definition of recovery? IDK, and I know nothing about those dynamics at Stanford. It just caught my attention and got me thinking. (More here.)
When you’re in recovery, your old methods of relieving stress – having a drink or using a drug – can no longer be utilized. It’s time to build new, healthier habits that allow you to relax and enjoy yourself while also improving your lifestyle and setting yourself up for future success in your recovery. Below are some tips for healthy stress relief that may seem like common sense, but are oven overlooked and undervalued.
- Do physical activities you actually enjoy. Fitness journeys look different for everyone – but most people will agree that exercise is a great stress reliever. That doesn’t mean you have to go overboard on the treadmill or lift weights at the crack of dawn. Find a routine that works for you, and you’ll be much more likely to stick with it and genuinely enjoy it. When you’re engaged in physical activity, your brain releases endorphins that make you happier. Exercises done daily such as yoga, aerobics, and even simply walking can go a long way towards making you feel better about yourself and your life.

- Maintain a healthy diet. Along with a good exercise regimen, a healthy change in diet will help prevent negative feelings and regret that accompany a junk-food binge. Again, this doesn’t mean you have to go overboard – take small steps to create a greater lifestyle change that you’re more likely to keep up with. When you eat healthier, your mood improves
- Build better sleep habits. “Eight hours a night” isn’t just something your parents made up – science shows that we are more productive, have better memory, and are overall happier when we fit enough sleep into our schedule. Running on less sleep leaves us ill-equipped to handle life’s challenges, which inevitably leads to a buildup of stress.
- Talk it out. Opening up certainly isn’t an easy task, especially for those in recovery who are used to isolating and self-medicating rather than speaking their mind when they’re struggling. In treatment, you discover how important and necessary talking about your feelings can be – don’t lose that ability once you’re in the real world. Continue having discussions with your loved ones and your recovery support network. Don’t keep anything bottled up. Your stress levels will drastically decrease as you get things off your chest and receive verbal support and feedback from those around you.
Remember that being kind to your body, no matter which way you go about it, is the best way to relieve yourself of stress, whether internal or external. When you practice healthy ways of coping with stress, you’re reinforcing those behaviors in ways that make you more likely to keep up with them, though they may seem difficult or tedious at first. As in recovery, stress relief is a constant battle that must be taken seriously and dealt with in healthy ways.
For more information, resources, and encouragement, “like” the Fellowship Hall Facebook page and follow us on Instagram at @FellowshipHallNC.
About Fellowship Hall
For 50 years, Fellowship Hall has been saving lives. We are a 99-bed, private, not-for-profit alcohol and drug treatment center located on 120 tranquil acres in Greensboro, N.C. We provide treatment and evidence-based programs built upon the Twelve-Step model of recovery. We have been accredited by The Joint Commission since 1974 as a specialty hospital and are a member of the National Association of Addiction Treatment Providers. We are committed to providing exceptional, compassionate care to every individual we serve.

Rob Russo (RobR62) found SMART Recovery several years ago and immediately clicked with the program. Six months in, he took the facilitator training and now facilitates three SROL meetings a week. Rob provides a space for other to connect and learn from one another in their continued path to recovery.
Learn more about becoming a SMART volunteer
Subscribe to the SMART Recovery YouTube Channel
Video storytelling is a powerful tool in recovery, and we are proud to share our SMART Recovery content free-of-charge, available anywhere, on any device. Our videos hope to inform, entertain, and inspire anyone in the recovery community.
Subscribe to our YouTube channel and be notified every time we release a new video.
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!
SMART Recovery is partnering with researchers from the University of New Mexico for a study on alcohol recovery. Using the PERMA Model, Positive emotions, Engagement, Relationships, Meaning, and Accomplishments, they will evaluate the profiles among individuals who self-identify as being in recovery from alcohol use disorder (AUD), to help bridge the gap between the fields of positive psychology and addiction.
Study participants:
- Must be 18+
- Must take the two, online surveys in English
- Must identify as in recovery from an alcohol use disorder
- Will receive Amazon gift cards totaling $30
The study is open until Monday, May 16, 2022 or when the 250 number participants is reached, whichever is first.
For questions, please contact: Lead Researcher, Hannah Carlon, [email protected]
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @ 800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!

Dr. Nora Volkow recently spoke to the SMART Recovery community about how the National Institute on Drug Abuse (NIDA) is taking a holistic approach to helping those with substance use issues through prevention, treatment, and after care. As a follow up to that conversation, we talked with Dr. Wilson Compton, Deputy Director of NIDA and Dr. Will Aklin, Director of the Behavior Therapy Development Program, about the research happening in the advancement of substance use treatments.
In this podcast, they talk about:
- How their college professors got them excited and passionate about careers in scientific research
- Medications that help with various addictions, including a new focus on stimulant use disorders
- Bridging the gap between treatment and recovery
- Individualized, personal treatments
- Examples of harm reduction measures
- Creating a net positive to society
- The four pillars of overdose strategy: primary prevention, harm reduction, and evidence-based treatment, and recovery support
- Explaining the value of CBT and MAT
- How research helps us understand the impact of mutual support and recovery
- The research behind using Contingency Management to shape positive behavior
- Making treatment less intimidating and more welcoming
- Working across boundaries and departments, within the government, to address the drug abuse problems and find solutions
Additional resources:
Click here to find all of SMART Recovery’s podcasts
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @ 800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!
Fellowship Hall, a 96-bed private, not-for-profit specialty hospital offering abstinence-based alcohol and drug treatment based on the 12-Step Model of Recovery, located on a serene 120-acre country setting in Greensboro, NC, is currently seeking a Part-time Evening Front Desk Receptionist to work Monday-Friday, 4p-8p. Fellowship Hall has been established for 45 years and enjoys a stellar reputation as one of the premier treatment providers in the country. Our facility has been accredited by Joint Commission since 1974, and we offer inpatient care, detoxification, partial hospital, intensive outpatient, family programming, extended treatment, and structured living. We draw our guests from North and South Carolina, Virginia, and 23 other States.
The Evening Front Desk Receptionist position is responsible for three primary areas:
• Reception activities including but not limited to: answering all incoming calls to the facility, registering all visitors and providing services to the guests such as making change, selling stamps, accessing the safe, etc.
• Assist the Admissions team with new admissions from arrival until they are admitted.
• General office work, including scanning of documents, insurance cards and IDs, creating door tags, tracking packages,
• Assist with COVID screenings and temperature checks for all staff and visitors arriving to campus during shift.
• Order supplies and manage inventory of supplies. Coordinate distribution of special request supplies.
• Supporting Accounts Payable duties by managing invoice approvals, entering invoices for payment, paying invoices, and managing any questions or concerns from vendors.
• Providing support to the Outreach Department by manning the online chat system during the evening hours
Minimum Education: High School Diploma
Minimum Experience: 3 Years as receptionist or customer service-related work
Preferred Education: Workshops and inservices in substance abuse
Skills: Telephone communication proficiency
Good interpersonal relationship skills
Computer skills, proficient in Excel and WORD
Good organizational skills, Ability to multi-task
Exceptional customer service skills, internal and external
High degree of professionalism
Independently self-productive
Teamwork and Collaboration skills
var gform;gform||(document.addEventListener("gform_main_scripts_loaded",function(){gform.scriptsLoaded=!0}),window.addEventListener("DOMContentLoaded",function(){gform.domLoaded=!0}),gform={domLoaded:!1,scriptsLoaded:!1,initializeOnLoaded:function(o){gform.domLoaded&&gform.scriptsLoaded?o():!gform.domLoaded&&gform.scriptsLoaded?window.addEventListener("DOMContentLoaded",o):document.addEventListener("gform_main_scripts_loaded",o)},hooks:{action:{},filter:{}},addAction:function(o,n,r,t){gform.addHook("action",o,n,r,t)},addFilter:function(o,n,r,t){gform.addHook("filter",o,n,r,t)},doAction:function(o){gform.doHook("action",o,arguments)},applyFilters:function(o){return gform.doHook("filter",o,arguments)},removeAction:function(o,n){gform.removeHook("action",o,n)},removeFilter:function(o,n,r){gform.removeHook("filter",o,n,r)},addHook:function(o,n,r,t,i){null==gform.hooks[o][n]&&(gform.hooks[o][n]=[]);var e=gform.hooks[o][n];null==i&&(i=n+"_"+e.length),gform.hooks[o][n].push({tag:i,callable:r,priority:t=null==t?10:t})},doHook:function(n,o,r){var t;if(r=Array.prototype.slice.call(r,1),null!=gform.hooks[n][o]&&((o=gform.hooks[n][o]).sort(function(o,n){return o.priority-n.priority}),o.forEach(function(o){"function"!=typeof(t=o.callable)&&(t=window[t]),"action"==n?t.apply(null,r):r[0]=t.apply(null,r)})),"filter"==n)return r[0]},removeHook:function(o,n,t,i){var r;null!=gform.hooks[o][n]&&(r=(r=gform.hooks[o][n]).filter(function(o,n,r){return!!(null!=i&&i!=o.tag||null!=t&&t!=o.priority)}),gform.hooks[o][n]=r)}});

Dr. Nora Volkow, the director of the National Institute on Drug Abuse (NIDA), recently published an article in Health Affairs Magazine that many in the recovery community consider “a game changer” in how it challenged received wisdom and old assumptions in the treatment of addicted individuals. In this interview, Dr. Tom Horvath, co-founder of SMART Recovery, assesses the article’s impact and how it may change the face of the recovery landscape forever.
Read Dr. Volkow’s article in Health Affairs Magazine
Subscribe to the SMART Recovery YouTube Channel
Video storytelling is a powerful tool in recovery, and we are proud to share our SMART Recovery content free-of-charge, available anywhere, on any device. Our videos hope to inform, entertain, and inspire anyone in the recovery community.
Subscribe to our YouTube channel and be notified every time we release a new video.
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!