

SMART Recovery is delighted to announce a partnership with The Fletcher Group to bring SMART Recovery into recovery homes in rural counties, as designated by Health Resources & Services Administration, the funding agency for this endeavor. This partnership enables SMART Recovery to increase our footprint in rural communities and fulfill our mission to empower people with limited access to achieve independence from addiction problems with our science-based 4-Point Program®. We are excited to bring these opportunities to our dedicated & amazing SMART experienced volunteers*.
A few of the key actions that SMART will undertake as part of this partnership are:
- Hire a full-time, paid Project Coordinator dedicated to the administration, coordination, planning, and setup of a SMART Recovery 12-session program, using the Successful Life Skills handbook in 100 recovery homes located in rural areas across the U.S.
- Recruit experienced SMART Recovery facilitators for each 12-session program.
- Provide training for up to 100 recovery home staff to become future facilitators of our SMART Recovery program, allowing them to continue offering SMART after the initial 12-week session has ended.
As a result of our partnership with The Fletcher Group, we are able to extend two unique opportunities to our volunteers*.
- First, we would like to invite qualified and experienced SMART volunteers to apply for the Project Coordinator position. The Project Coordinator will be the lead contact and will be working closely with the Fletcher Group Project Coordinators and Administrators as well as the assigned program coordinator of each of the 100 recovery homes. Their primary responsibility will be to effectively align and manage all needed resources to ensure the successful planning and execution of the 12-week meeting programs. This will include effective scheduling coordination for all participating recovery homes and SMART resources, budget oversight to maintain pre-approved expenditures, technical support, meeting delivery, evaluations to help reach the goals and deadlines of the project, and occasionally filling in on an as-needed basis as a meeting facilitator. This position reports directly to the Executive Director and Assistant Executive Director but will work closely with SMART Volunteer Managers. CLICK HERE to view the full job description, requirements, and application process.
- The second opportunity is for facilitators who would like to be part of getting these 12-week sessions started. Ideally, we would like to have teams of 1-3 facilitators to run the first 12-week session at each of the 100 recovery houses. The meetings will be hybrid and can be held through Zoom and/or a physical location. We do not anticipate all 100 meetings starting at the same time, but rather be staggered throughout the year. If you are interested in facilitating one or more of these 12-week sessions, please fill out this form.
*These opportunities are for volunteers in the U.S. only.
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @ 800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!

I must have signed tens of thousands of prescriptions over the years for a variety of medical conditions from athlete’s foot to diabetes. Not one patient, as far as I can remember, has congratulated me on my expertise around knowledge of the evidence base, guideline awareness, titration skills, dose precision, grasp of pharmacodynamics or knowledge of drug interactions. Important and necessary as all of these are, these things are often valued more by science than they are by patients.
Don’t get me wrong – I respect medication and its impact. People’s lives often improve because of what we prescribe, but when people have fed back to me after meds have been started, the take home message has not been about the medication. The patients I work with rank other things higher than the prescription and even its impact.
It is the anecdote that connects us to our patients, it is understanding the individual for whom we care that brings us joy, and it is connecting with their personal experiences that makes our work so rewarding.
Meagan Brennan
What I’ve learned from patient feedback is that certain values – listening, empathising, caring, and taking time with them – are far more valued than the drugs I prescribe, regardless of what the evidence base says. Sometimes the medication does not work the way we hoped it would and sometimes it does. While many medications are undoubtedly effective, generally I believe we doctors tend to over-value what a pill, cream or liquid can do. I certainly have done – many times. However there are other things in our meetings with patients that have value and these are not always recognised.
We make treatment plans for patients using the latest drugs. Usually they work well, but when they don’t, we label the patient “non-compliant.” After all, they must be doing something wrong because we have enacted an “evidence based” plan.
Meagan Brennan
In her blog[1] for the BMJ, Meagan Brennan raises the concern that as we focus more and more on the evidence, we lose the humanity that is essential for good care and outcomes. She points out that the promising-sounding ‘personalised medicine’ that is now being introduced, in fact, takes us further from ‘the heart of doctor-patient interactions and deeper into the realm of impersonal science’.

She lauds the new interest in the humanities that is developing in medical student teaching. I remember so strongly when I was at medical school missing the subjects I had studied at school that had nothing to do with science. I was missing out on things that inspired me and sent my imagination and creative spirit soaring. Dealing with suffering, the impact of trauma, the bleakness of illness and death – and what those things actually mean – was not something I was prepared for in any way by my scientific training at university. In fact during a six month hospital job in a cancer unit, I almost gave up on medicine as a career. My spirit had been diminished by watching the suffering my patients experienced – sadly a significant number were to die despite the best treatment available. I wasn’t able to admit it at the time, but I was frightened and out of my depth. My difficulty in dealing with this was not unique but this simply wasn’t something we junior doctors were encouraged to talk about. Several decades later I find myself considering the question raised by Brennan: could the study of medical humanities have helped?
Medical Humanities: Its advocates contend that it can develop empathic practice and a social justice conscience in medical students. It is also being explored as a tool to enhance job satisfaction and reduce burnout in consultant physicians and junior doctors.
Studying the medical humanities can help doctors gain insight into what illness means for patients, but crucially can increase self-awareness and self-perception. The subjects that come under this banner take in concepts like relationship, emotion, the narrative, and spirituality. While medical humanities may help us humanise our own and our patients’ experiences, stigma does a very effective job at doing the opposite.

In another paper[2] by Harry Sumnall and colleagues, the dehumanising of heroin users is evidenced – framing those who use heroin as different, less worthy, and even ‘disgusting’. People who use heroin become less than human and more animal-like. Such characterisation is associated with ‘moral disengagement’ and distancing by others and can have real-life consequences including the ‘denial of human agency’ in popular and political discourse. This can lead to reduction of treatment funding when policymakers rationalise that due to lack of public support, there will be little protest when resources for addiction treatment are slashed. Many of us experienced harsh cuts to treatment services not that long ago. I remember thinking that cutting paediatric or cancer services to that degree would have been seen as unconscionable, yet it happened in addictions.
How do Sumnall and colleagues think dehumanising should be tackled? Simply, as it turns out: by social inclusion and by humanising narratives. Letting people tell their stories in the media – ‘encouraging compassionate media representations’ is likely to humanise. After all, listening is a two-way street. My listening to my patients is appreciated by them, but the same process has the power to change the way I see their world – how I perceive and relate to them.
The topics of humanising and dehumanising are ultimately about relationship and connection, or lack of it. When I am connected to you, I see your humanity – I value you more and draw closer. In a doctor/patient relationship this may be expressed as commitment. My determination to support you strengthens the more connected to you I become. This process needs healthy boundaries to be effective, but many of us can find ourselves distancing from pain and suffering because of the emotional cost of connecting. My frightened junior doctor self did not recognise that although I could not save every life from cancer, I was doing something meaningful by being present, listening and connecting. Perhaps this represented being spiritually available.
Mark Galantar and colleagues frame deeply felt commitment as a spiritual component in the recovery process which in itself adds to recovery capital – the resources people can call upon to help them resolve their problems and recover. In a paper about spirituality in addiction medicine[3] they point out that recovery can signify finding ‘meaning and purpose in life’.
“Spirituality has been defined with regard to clinical settings as a commitment to transcendent or existential personal meaning in one’s life, typically involving a connection with something larger than oneself and is distinguished from the pursuit of material needs or organised religion”.
Galantar et al
Galanter et al reference the strong evidence behind the spiritual approach of 12-step groups citing the recent Cochrane review on Alcoholics Anonymous, and although they point to neuro-imaging research that may support the potential benefits of spirituality, they also highlight that the dominance of a biological/medication perspective is often at the expense of integrative approaches which acknowledge the ‘interconnections of mind, body and society’.
“Abstinence after discharge from professional treatment was found in one study to be three times as likely among patients who reported having had a spiritual awakening”.
Galantar et al
They assert that spirituality is often ‘culturally resonant’ with underserved or disadvantaged groups and that ‘engaging spirituality and related community organisations in treatment is an important aspect of improving treatment access, outcomes, and equity for underserved groups’.
Addiction, the behaviours associated with it, society’s stigmatising attitudes and the shame that so many people carry with them as a result, can result in dehumanising attitudes and responses. Studying the medical humanities may help current and future doctors be better physicians and to be more connected to themselves and their patients. Hard science alone cannot provide us with all of the tools that we need – a spiritual dimension is also required.

Everyone will have their own understanding and experience of ‘spirituality’, but in my practice, I think of it simply as things that enrich my spirit – that make me spirited. When my spirit is quickened, then I am a better doctor. Listening to patient narratives – ‘what’s happened to you?’ – finding meaning in those stories, putting judgement aside, empathising with the individual, connecting with that person in front of me and meeting them where they are – are for me deeply spiritual things. Others may choose to call the same things something more scientific – a complex interaction between oxytocin, serotonin and dopamine perhaps, but I find myself resisting that urge.
What if, as Meagan Brennan suggests, we are missing a piece of the evidence in our evidence-based practice? What if this something is both profound and necessary? Whether we call it humanity, connection, spirituality or something else, the amazing thing is that by adding this in and truly listening to our patients’ stories we will help not just them but ourselves too.
To be a good doctor you need to have a robust grasp of the science of medicine, but that’s not enough in itself. We need to come alongside our patients, draw close and travel a bit with them. Listening compassionately to their story is the way to do this. When the day comes that I hang up my stethoscope for the last time, my hope is that I am not so much remembered for my prescriptions or my medical expertise (such as it is) as I am for my humanity.
Continue the discussion on Twitter: @DocDavidM
[1] https://blogs.bmj.com/bmj/2021/09/02/are-we-losing-our-humanity-in-medicines-quest-for-pure-science/
[2] Sumnall, H., Atkinson, A., Gage, S., Hamilton, I. and Montgomery, C. (2021), “Less than human: dehumanisation of people who use heroin”, Health Education, Vol. ahead-of-print No. ahead-of-print. https://doi.org/10.1108/HE-07-2021-0099
[3] Galanter M, Hansen H, Potenza MN. The role of spirituality in addiction medicine: a position statement from the spirituality interest group of the international society of addiction medicine. Subst Abus. 2021 Jul 2:1-3. doi: 10.1080/08897077.2021.1941514. Epub ahead of print. PMID: 34214398.

The topic of this article concerns defects in the alcoholic family system that are caused by the birth of a well baby. This article is not about defects found in a newborn.
As we consider the topic of defects in the family system, for the purposes of this article, let’s consider the family system as one whole solid object.
Sometimes the idea of a planned child is that the arrival of the new family member will repair the alcoholic home.
But we know that the birth of a newborn is a stressor for any family system – alcoholic or not. And we know that in some families the arrival of and ongoing presence of a newborn degrades the function or structure of the family system, or both.
I would like to suggest that the stress brought by the newborn’s arrival might finally bring the pressure necessary to create a fundamental crack or break (a basic fault) in the structure of the alcoholic family system. This can be thought of as creating a new seismic fissure or fault in the totality (or whole) of the family system.
This stress in a home with active alcoholism or a home without sufficient recovery stability could cause a fracture in the basic structure of the family system. And that could leave the family system forever weakened and unsafe for others.
A metaphor for the family system
One metaphor or image commonly used to capture the idea of a family system is that of a mobile, with each part of the mobile representing a different member of the family. And showing the mobile as out of balance is the way a problem in one of the people, or in the system, is shown.
But for this concept the image would not be that of a mobile. Rather, the image is that of an entire solid granite continental shelf a few miles thick. And the problem being shown is represented as a deep break – a new fault. And the break is caused by a new pressure (such as a new birth) – that would normally be thought of as both normal and good.
Extending the metaphor or image of a one-piece solid geologic structure, we should recognize at least two possible problems other than a new deep break exist. The first is that within some families the added stressor would simply make the defects that already existed in the system visible for perhaps the first time. And in other family systems the added stressor would simply make an existing break larger.
Questions include:
- Why does the topic of “birth defects” seem to always and only pertain to defects in the person of the newborn infant? And why do we have such a limited perspective from which to view the situation?
- Can our thinking also pertain to new malformations in the family system as a whole?
- What newly emerging defects of the family system threaten the newborn’s health and well-being? And for how long?
- In our clinical work do we examine the integrity and stability of the family system?
- Do we help the family system accommodate the positive pressures of its existing members, new members, returning members, members shifting into abstinence, and members shifting into recovery?
From ACES to Recovery Capital
This causes me to wonder if we can apply the list of Adverse Childhood Experiences Survey (“ACES”) in a positive way. Such an effort could help us reverse the concept of ACES and identify the features of a healthy-enough recovery community at various social levels, starting with the family system.
What is good enough “parenting”?
- For the alcoholic home to aspire to?
- For the abstinent home to aspire to?
- For the recovering family to aspire to?
- For the recovery community to aspire to?
Conclusion
If our babies break us, are we a “healing forest”? Or are we only looking at the trees?
To help anchor these concepts and areas of attention we could coin new terms.
- One term would be for the problems in the family system caused by the arrival of a newborn. Perhaps for this phenomenon we could coin the term “Birth-related family system defect”.
- And we could coin a term for the permanent damage in the actively addicted family system, or the newly abstinent but not recovering family system, caused by the pressures brought by the birth of a newborn. Perhaps that term could be “Fetal recovery syndrome”, given it is the new life present in the new person of the infant that in some cases seemingly deforms the family.
Can we improve our systems of care for chronic, severe, and complex substance use disorders to include evaluation, positive change, and on-going recovery support of the entirety of the family system until the critical threshold of structural instability is resolved?
Suggested Reading
Balint, M. (1969). The Basic Fault: Therapeutic Aspects of Regression. Northwestern University Press.
Coon, B. WHERE is Addiction? July 8, 2021. Recovery Review.
Coon, B. We All Need to Learn “Prevention”. August 13, 2021. Recovery Review.
Herzog, J. I. & Schmahi, C. (2018). Adverse Childhood Experiences and the Consequences on Neurobiological, Psychosocial, and Somatic Conditions Across the Lifespan. Frontiers in Psychology. doi: 10.3389/fpsyt.2018.00420
Swedish Agency for Health Technology Assessment and Assessment of Social Services. (2016). Fetal Alcohol Syndrome (FAS) and Fetal Alcohol Spectrum Disorders (FASD) – conditions and interventions. sbu.se
Touloumakos, A. K. & Barrable, A. (2020). Adverse Childhood Experiences: The Protective and Therapeutic Potential of Nature. Frontiers In Psychology. doi: 10.3389/fpsyg.2020.597935
White, W. (2011). Unraveling the mystery of personal and family recovery. An interview with Stephanie Brown, PhD.
Winnicott, D. (1974). Fear of Breakdown. International Review of Psycho-Analysis. 1(1-2): 103-107.

SMART Recovery is proud to support Sober Voices for FLOW.
This international event is open to those in early sobriety, sober-curious, and in long-term sobriety of any kind.

The four days will be filled with content from a diverse array of leaders in the sober movement. Among them will be Mike Hooper, SMART’s State Outreach Director for Ohio, who will be speaking during the event.
For more information and to purchase tickets, go to: https://flow.sobervoices.co
Use to the promo code SMARTRECOVERY50 to save 50% off the ticket price.
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @ 800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!
Bill White recently wrote a powerful post about the intersection of recovery, character, and activism. First, on character as an essential element of recovery advocacy:
What is the role of character reconstruction in addiction recovery? In recovery activism? I have repeatedly returned to these questions over the course of my adult life, especially as young recovery advocates sought my guidance on how to best use their lived experience as a catalyst for social change. Effective recovery advocacy and peer recovery support depend on the scope and depth of one’s knowledge and skills, but equally important is this dimension of personal character.
He goes on to explain that advocacy founded on personal character requires a personal mission and code:
The challenge in recovery is how to rebuild a name (character) ravaged by the addiction experience. The challenge in recovery advocacy is how to use the fruits of that character reconstruction as a fulcrum for one’s service to others. As Burroughs suggests, service to one’s cause requires a foundation of personal integrity. That, in turn, requires a personal mission/vision (What am I here to achieve?) and a personal code (What are the values and personal code that will guide my journey toward that goal?)
Bill shared his own mission/vision and code, which I strongly recommend you read and reflect upon. It includes maintaining his own recovery, emphasizes listening to others, seeking to understand people who offend him, humility, and supporting the freedom of the people he seeks to serve.
He follows his own code with this statement:
Such an actionable set of values constitutes the building blocks of character. It enriches the recovery experience, quiets the childish attention-seeking of the self-absorbed ego, and enables compassion and care for others.
The post is worth reading, contemplating, and re-reading.

Sarah Levin is the founder of Secular Strategies. She is also a lobbyist and coalition builder. Sarah has made it her life’s work to fight for legislation protecting secular points of view.
Gerardo (Gee) Matamoros is a SMART Regional Coordinator, president of the SMART NYC Board, and self-described newfound activist. He is impacting his community through his passion and dedication to ensuring SMART is an option for everyone in recovery.
In this podcast, they talk about:
- Sarah growing up in a political family that loved to talk about religion and politics at the kitchen table
- Sarah being introduced to SMART when she worked for the Secular Coalition for America
- Being the engine of the secular movement
- Gee grew up in different countries and came to the US for college
- Gee’s stint with “naughty” substances and finding SMART
- What brought Sarah and Gee together
- Advocating for separation of church and state and evidence-based policy
- Explaining to law makers why Medically Assisted Treatment (MAT) should be supported in recovery
- Ending the stigma of addiction for people in recovery
- The First Amendment cases that protect choice in recovery pathways
- Shifting the burden to the courts to ensure secular recovery options are given to people
- Gee’s outreach and awareness efforts in NYC
- Newfound energy in rallying people to get involved in SMART’s legislative changes
- Why it’s important to learn the ecosystem of decision makers in your community and make SMART known
- Telling your story because your voice matters to lawmakers at all levels
Additional resources:
Click here to find all of SMART Recovery’s podcasts
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @ 800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!

Pete Rubinas found SMART Recovery when he observed someone close to him transforming their life using SMART tools and techniques. That led Pete to examine his own relationship with alcohol, and he decided to build a new balanced alcohol-free life without it with the help of fellow meeting participants.
As part of giving back to a program that helped him live his best life, Pete started facilitating regular SMART Recovery meetings before helping to found the first local SMART Family & Friends meetings in the Triangle region of North Carolina. He’s gone on to become the SMART Regional Coordinator for North Carolina, supporting other facilitators around the state as they strive to provide compassionate support to those struggling with an addictive behavior.
Learn more about becoming a SMART volunteer.
Subscribe to the SMART Recovery YouTube Channel
Video storytelling is a powerful tool in recovery, and we are proud to share our SMART Recovery content free-of-charge, available anywhere, on any device. Our videos hope to inform, entertain, and inspire anyone in the recovery community.
Subscribe to our YouTube channel and be notified every time we release a new video.
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!

When the news of Scotland’s 2020 alcohol-specific deaths – all 1190 of them – was published last month, I was fascinated to compare the reaction in the press, TV and social media to the respective reaction after the publication of the drug deaths. Our ‘other’ drug deaths, quite rightly, provoked outrage, grief and calls for change. To me the response to the alcohol deaths seemed like a whimper rather than the bang such loss deserves.
Beyond the terrible impact of those deaths is the astounding cost of alcohol harms to the Scottish economy. In 2010, the Scottish Government estimated that the cost of excessive drinking here is around £3.6 billion when social, criminal justice and health factors are considered. The fallout in families and communities is considerable.
When we were exploring access problems to residential rehabilitation in Scotland, the Residential Rehabilitation Working Group did not find any evidence that access for alcohol problems was any better than for drug problems, yet there has been little energy spent on trying to increase access for this group.
Given that there was a 17% year on year increase in fatalities and that the number of alcohol-specific deaths is a significant underestimate of deaths in which alcohol plays a part, I wondered in a tweet why there was a more muted reaction to the alcohol deaths than to the drug deaths. This touched a nerve it seems. A lot of responses were generated and I wanted to share some of the themes here.
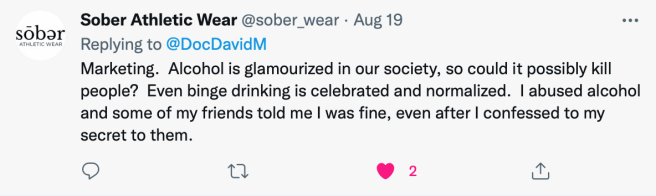
Fred Parry, who recently made a poignant plea for more action on alcohol addiction in the Ferret makes the salient observation that there may be a degree of denial going on because alcohol is society’s ‘drug of choice’. Several commentators picked this theme up including Steven R.
The way alcohol is seen and the allowances made for it are relevant to this debate:
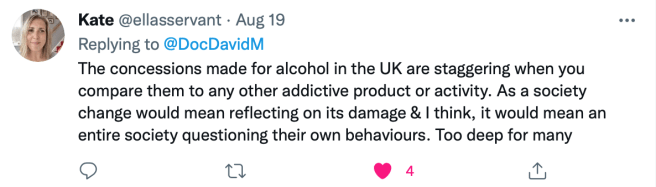
I am pretty much in agreement with Emma Rogan:

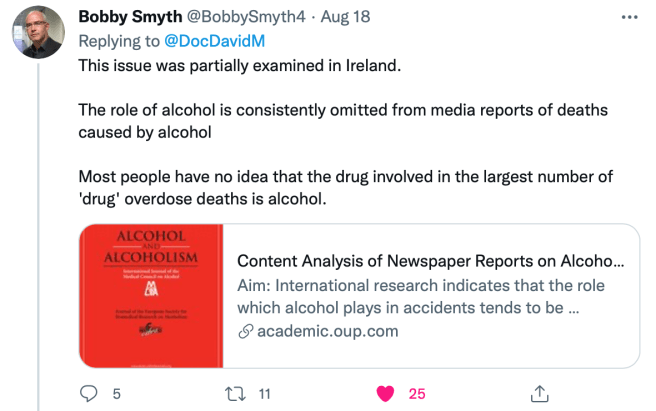
And do the press collude in keeping attention deflected? Bobby Smith thinks so:
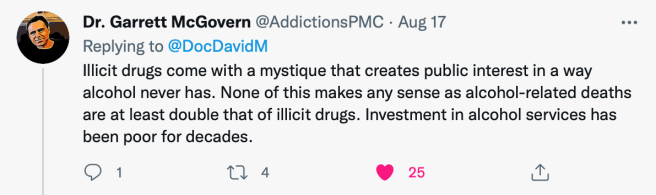
There was emphasis on the contrast of the legal drug alcohol with illicit drugs, perhaps meaning we pay less attention. Perhaps too, the illicit nature of other drugs creates a glamour/mystery which causes more of a splash. My colleague, Garret McGovern picks this up, also :
The idea of underinvestment in alcohol services was challenged by Andrew McAuley:
It’s true a lot of effort has gone into policy – we have national minimum unit pricing and alcohol brief interventions, but what about treatment? Peter Rice had a different perspective:

This raised for me the unwelcome thought: what if our understandable emphasis on tackling drug deaths was having the unintended consequence of our neglecting of alcohol deaths?
Perhaps the ferocity and immediacy of other drug harms are relevant:

And does tax revenue and lobbying from the alcohol industry have a part to play in our dulled response?

I wonder too if part of the problem is the swing of the pendulum. We have trouble with multitasking – at points in the past, the emphasis has been on alcohol. At the moment it’s more on other drugs – perhaps it will swing back, though what we really need is a mid position where we give alcohol problems and their prevention, harm reduction and treatment the same priority as other drugs. You can see many more comments here.
For the moment though, for the sake of all those suffering and dying prematurely – and their families, I think we need not the whimper we got in response to alcohol deaths but a very loud bang instead.
Continue the discussion on Twitter @DocDavidM
Note: I’ve not sought permission to publish these tweets as they are already published in the public record, – but if anyone would like me to remove their comment, please let me know. Thanks to all who took time to comment on the Twitter thread.

Join SMART Recovery on September 24-26 for our first-ever, nationwide Pathways to Recovery walk. This virtual event is sure to provide a day of reflection, exercise, and fun. In addition, your fundraising efforts will enable us to help more people who are on the path to recovery find life beyond addiction.
There is no RIGHT way to recover. Individuals who choose their own pathways to recovery are more likely to move from a life of substance misuse and self-harm to a life of positive self-regard and willingness to change. Supporting and celebrating this idea of multiple pathways to recovery is what our new event, Pathways to Recovery, is all about.
About the Pathways Walk
- Choose your own 1+ mile path
- Walk anytime on the weekend of September 24-26
- Participate alone or with your family and friends
- Take pictures with the hashtags #multiplepathways and #SMARTRecovery, and tag SMART Recovery on our various social media platforms
How to Participate
REGISTER
Register by September 23 to take part in our virtual Pathway to Recovery walk, the weekend of September 24-26.
SUPPORT A FUNDRAISER
Donate to a personal fundraising page to support the “Pathway to Recovery” event.
PAVE THE PATH
Help us pave a virtual path to recovery! Buy a virtual brick in honor or memory of a loved one or to honor a hero in your recovery journey.
Questions, please contact giving@smartrecovery.org
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to The National Suicide Prevention Hotline @800-273-8255, https://suicidepreventionlifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Subscribe To Our Blog
Join our mailing list to receive the latest news and updates from the SMART Recovery Blog.
You have Successfully Subscribed!
When the Doctor Is In… Treatment: When Helpers Need Help

What happens when those who treat, support, heal, or educate need treatment, support, healing, and education of their own? This is a question that many professionals are negotiating when they enter treatment for their own experience of addiction disease. As we know, addiction disease does not discriminate. It is an equal opportunity illness which means that anyone— regardless of his or her professional successes— is susceptible to its emotional, physical and spiritual destruction. In working with lawyers, physicians, pharmacists, physicians’ assistants, counselors, executives, and educators there are some issues that arise for professionals that are (but don’t have to be) unique.
Look at what I have accomplished, how could I possibly be addicted?
For many professionals, the dissonance created from a lifetime of academic and professional successes in the face of addiction disease can be difficult to negotiate. At times, the unmanageability of addiction is glaringly obvious and has spread to a professional’s work life. This can include legal problems, complaints filed with the professional’s board, or job loss or demotion. In other circumstances, the professional has been able to keep his or her work life largely intact. As professionals begin to expand their awareness of the breadth of their lives to include relationships, emotional and spiritual worlds, the impact of their addictive process becomes clear. Often professionals find that as they tend to the disruption addiction has created in these areas of their lives, their professional successes could not ease the emotional and spiritual wounds they have been carrying since long before they were addicted. By addressing this relational and emotional unmanageability, professionals find more meaningful and fulfilling relationships with patients, clients, colleagues, and family members that are mutually supportive of one another in both recovery and beyond.
How am I supposed to be the patient or client?
The old adage that “doctors (or nurses and healthcare professionals) make the worst patients,” holds a kernel of truth. As professionals make the transition from offering direction, care and/or advice, to being the recipient of such direction and care, it can naturally be a jarring and uncomfortable transition. Learning how to give oneself permission to not know and to be helped and cared for can offer professionals much needed relief from the pressure of high stress expectations. Allowing oneself to be vulnerable to support gives professionals permission to be human when often their professions demand perfection. Many times, professionals find that they have looked to alcohol and/or drugs to provide them with the exact relief that is found through the acceptance of the support available in a treatment and recovery environment.
What if I see a patient or client in a meeting?
The more accurate question is not “if” but “when.” An entire essay could be written about all of the “what if” scenarios that can occur at Twelve Step recovery meetings. Shame says that patients and clients will “think less of me, avoid me, or stop seeing me if they see me at a meeting.” The reality is that the opposite is more often the experience. Patients and clients feel understood, seen, and heard by professionals with whom they can relate and see as equals. Many recovering people seek out professionals who understand addiction and the importance of recovery, as they feel safe to share openly about their history.
How can I fit meetings into my work schedule – especially when I have been gone for so long?
This issue often involves a significant paradigm shift for professionals whose priority has been work and career— often at the cost of self-care and personal relationships. Many times, organizational and professional expectations compound this belief to the detriment of its employees. This reprioritizing can begin through external support (monitoring entities or restricted practice) and eventually become internalized to support long-term recovery efforts. Professionals, like others in recovery, can start with the acceptance that because of active involvement in recovery, aftercare and individual counseling, meetings, connections to others in recovery, a full life is available. It is because of the hard work that occurs during treatment that continuing to be in one’s chosen field is possible. By tending to recovery first, professionals are able to teach colleagues, patients, and mentors about the need to take care of self, first… and then others.
How do I talk with my colleagues about where I have been?
It depends. Working professionals returning to work after a lengthy and/or unexpected absence can feel internal pressure to either over-disclose or simply avoid the topic all together. It seems that the closeness and safety of the relationship really dictates the nature of the disclosure. Professionals who are involved with monitoring boards have access to a wealth of guidance and support that can be helpful in negotiating these conversations. At times, mentors who are also in recovery, are available to help professionals as they transition back to home and work, from treatment. This kind of peer support is invaluable. Many professionals find enormous and unconditional support from close co-workers and colleagues who have been gravely concerned unbeknownst to the professional in treatment. In other circumstances, keeping any discussion at all short and vague is best. For colleagues, asking “How are things going for you since I last saw you?” is always a good option as most people are happy to talk about themselves.
The path of recovery.
While some of the issues that professionals address in treatment are unique to their high pressure, success-driven careers, the solution is the same as for those who may be unemployed, under-employed or have low-stress, easy-going jobs: connection and vulnerability. These two experiences offer all recovering people a safe harbor to find self-acceptance, community, and humanness. A place to create a full and fulfilling life that offers joy and hope to all of those who seek it.
Contributed by Mahala Motzny, Counselor
About Fellowship Hall
Fellowship Hall is a 99-bed, private, not-for-profit alcohol and drug treatment center located on 120 tranquil acres in Greensboro, N.C. We provide treatment and evidence-based programs built upon the Twelve-Step model of recovery. We have been accredited by The Joint Commission since 1974 as a specialty hospital and are a member of the National Association of Addiction Treatment Providers. We are committed to providing exceptional, compassionate care to every individual we serve.