

“. . . the individual, family and community are not separate; they are one. To injure one is to injure all; to heal one is to heal all. – from The Red Road to Wellbriety, 2002” – as quoted by William White, Recovery Rising
Perhaps the most important insight in recent recovery history is that recovery community, through collaborative effort leads to restoration not only in individual lives but supports healing across entire communities, in all their diversity. Recovery capital is a function of self and community agency. We saw that insight take form twenty years ago, highlighted in the writings of Bill White, Don Coyhis and many others. Bill wrote about recovery rising and community as the primary change agent of healing. Don wrote about incorporating native community methods into healing processes. Not narrowly defined peer service, but the capacity of community to heal itself. It works across America in modestly supported pockets. Developing recovery capital is fundamentally about resourcing and supporting diverse communities to address their own needs. This meets a lot of resistance.
We need to examine these headwinds if we are to keep moving forward. It is critical to take a hard look at how the recovery community gets sidelined and coopted in subtle or not so subtle ways. Head winds that create barriers to self and community agentry must be fixed if we are to get more Americans into wellness. These forces often stem from homeostasis, even as the state of things is woefully inadequate to the tasks at hand.
If we can reach a point where our voices are included in matters about us, our communities are strengthened, and we have real equity in the systems that serve us, headwinds can become tailwinds. To change, people and systems alike must come to terms with the impact of stigma on our recovery community. We must acknowledge that stigma of addiction and the discounting of persons with lived experiences is commonplace across all of our institutions. Stigma in the SUD realm often plays out across four interrelated dynamics:
- Cultural appropriation – The inappropriate or unacknowledged adoption of an element or elements of one culture or identity by members of another culture or identity. This is particularly true in respect to marginalized groups, which include the recovery community. Recovery initiatives not grounded in recovery are titled and run as such; treatment organizations rebrand services as recovery oriented for funding. Projects to collect our stories by outsiders are funded. Foundational elements of the recovery movement get appropriated when they become valuable. This extends to the very notion of recovery and all of its facets.
- Colonization – The action or process of settling among and establishing control over an indigenous people (in this case the recovery community). Control over what happens in the environment is delegated by entities in power to groups outside of the indigenous community to sustain control. This serves to undermine and inhibit the capacity of the inhabitants of recovery community to manage their own healing.
- – Healing methods and those permitted to provide such services shift away from the very recovery community who developed them. Barriers are erected to keep the marginalized group out in ways that the dominant group does not want or to prevent any shift of power to the marginalized group. Services become harder to provide. These barriers have the most severe and disparate impact on persons who are members of other marginalized groups, like BIPOC recovery communities.
- Cooptation – People from outside of recovery community organizations are placed in power over the role and function of recovery community groups to maintain the status quo. This serves to keep the recovery communities from developing a greater degree of agency over their own healing.
These are serious concerns not often spoken about in open dialogue out of very real risks of retribution but commonly discussed behind closed doors within the recovery community. Over the years, I have spoken to people around the nation in the recovery community who talk about how these dynamics play out. They include:
- Events or services initiated by the recovery community get taken over by treatment agencies or the government. We end up fighting to retain even window dressing levels of inclusion in our own projects.
- Pedagogy developed by us and for us get taken away and end up under the control of our bureaucracies, who then place barriers for us to access these very same methods of instruction. The process of learning and service provision begins to replicate the very challenges that they were developed to navigate around.
- Recovery communities are disparately resourced, instead academic, and large human service organizations get the lion share of resources. When funding is set up for us, recovery community groups are often pitted against each other for scraps. This creates further divisions that sustains an unhealthy homeostasis.
- Who has control over our stories matters! Our stories get clipped into other groups agendas. We get written out of our own history. Our stories must be handled in ethical ways. Communities who are written out of their own teachings cease to exist in a generation. Revisionist history replaces the authentic history.
Even the most well-intentioned policy makers often end up unintentionally reinforcing these dynamics. Stigma is that powerful and that entrenched. If you are in a position of authority over our communities and you see people asking a lot of hard questions or becoming upset by what you are doing, perhaps share some of the power and strive to understand it and seek remedy in collaborative ways to strengthen agentry. The more common reaction is to quash it. Shut it down and move the process forward to meet predetermined objectives.
Signs of affirming recovery community agentry:
- Systems that affirm our very right to define ourselves and keep in check ever-present tendencies to define and control us have a better opportunity to effectively strengthen recovery through collaborative action.
- Systems accountable to those of us they serve and open to this responsibility with a sensitivity to the most marginalized subgroups can augment our strengths, engender trust and lead to more effective outcomes.
- As Recovery Capital is a function of community and is not just and individual process, systems that ensure that resources get to the members of the community are telegraphing that they understand communities are best suited to affect their own healing. The opposite of paternalistic care, which is rooted in stigma.
Last year, I did a series of interviews with some of the pioneers of the New Advocacy Recovery Movement. One of the parts of the interview with Bev Haberle that resonated with me as fundamental in a recovery-oriented change processes is the centering of our efforts in community grounded ethics. During this interview with Bev, when I asked what she was most concerned about in respect to the future, she expressed a concern that we may end up falling backwards if not careful to pay attention to ethics grounded in the community served. She noted:
“I recall one of the Recovery Community Centers I was involved with and how much effort we put into building an authentic advisory group. People who served on this advisory group / vision team were charged with keeping us focused on the needs of the community and making sure everything we did was done with high ethical standards. They were charged with being stewards of quality recovery support services that meet the needs of the local Community being served. There was a lot of open discussion about what we were doing and we worked hard to make sure we stayed true to our community mission. They often spotted things the rest of us missed. People coming into our centers with what on the face of it looked like beneficial things but who had hidden agendas or self-dealing schemes. As a leader, I knew we needed them as our anchor to our mission.”
Well-functioning systems spend a lot of energy examining ethics and making sure that they run in adherence to good principles. Even the best-intentioned systems do unintentional harm, but the best of them actively work to minimize and fix those harms. In Pennsylvania, we have horrific examples of disparate treatment of the recovery community. It happens in other states as well. What harms one of us harms us all. I see recovering people leaving our field in droves because of the impact of moral injury, as I noted in this article in Treatment Magazine last May:
“Being in recovery makes many of us “those people” who end up getting disparate care. Every time I see it, I recognize it could be me getting disparate care and insurmountable barriers to accessing help. I could have ended up in a body bag instead of having a life. Every single day this very long week, I have spent time on the phone with people describing care denials of life-sustaining medical interventions under the lens of seeing addiction as a moral failing by licensed medical professionals, persons in long-term recovery who are being denied employment for decades-old legal charges and more. It is a normal week. It also hurts my soul.”
Disparate treatment creates systemic wounds that require healing. Healthy systems welcome tough dialogues and seek healing solutions to these wounds, dysfunctional systems shut down those discussions as too difficult and end up causing even deeper scars. What harms one of us harms us all. What heals one of us heals us all. These are tough subjects, but the work to heal these wounds can shift our headwinds to tailwinds and help heal whole communities. Ignoring these wounds deepen these harms and prevent collective healing. What kind of system of care do we want? The one I want to create deals with the tough stuff head on. If this was an easy process, we would have fixed it decades ago, it remains the challenge before us.
The question of how to describe and categorize addiction has been the subject of several of my recent posts. Some people scratch their heads about why I care so much about whether we think of it as a disease. Bill White summarized the stakes well here:
If AOD problems could be solved by physically unraveling the person-drug relationship, only physicians and nurses trained in the mechanics of detoxification would be needed to address these problems. If AOD problems were simply a symptom of untreated psychiatric illness, more psychiatrists, not addiction counselors would be needed. If these problems were only a reflection of grief, trauma, family disturbance, economic distress, or cultural oppression, we would need psychologists, social workers, vocational counselors, and social activists rather than addiction counselors. Historically, other professions conveyed to the addict that other problems were the source of addiction and their resolution was the pathway to recovery. Addiction counseling was built on the failure of this premise.
White, W. (2004). The historical essence of addiction counseling. Counselor, 5(3), 43-48.
Whether we define alcoholism as a sin, a crime, a disease, a social problem, or a product of economic deprivation determines whether this society assigns that problem to the care of the priest, police officer, doctor, addiction counselor, social worker, urban planner, or community activist. The model chosen will determine the fate of untold numbers of alcoholics and addicts and untold numbers of social institutions and professional careers.
The existence of a “treatment industry” and its “ownership” of the problem of addiction should not be taken for granted. Sweeping shifts in values and changes in the alignment of major social institutions might pass ownership of this problem to another group.
White, W. L. (1998). Slaying the Dragon: The History of Addiction Treatment and Recovery in America, page 338
I’ll acknowledge that hustles like patient brokering, cash MAT clinics, drug screen scams, and over-priced residential with little continuing care make it difficult to root for the survival of the “treatment industry” but White’s words capture the risks of transferring responsibility to other groups.
What’s made addiction counseling unique has been the emphasis on recovery as the endpoint. More specifically, a model of recovery that results in people with addiction becoming “better than well.”
An essential step in transferring responsibility from one group to another is redefining the problem.
Some efforts to define addiction as something other than a disease argue that it’s not a disease but, more often, arguments against the disease model are more about achieving particular goals (protecting liberties, assigning personal responsibility, advancing particular drug policy goals, advancing social justice, emphasizing particular interventions, stigma reduction, etc.) rather than questioning whether it’s actually a disease.
Recently, the American Journal of Public Health published an article titled The Harms of Constructing Addiction as a Chronic, Relapsing Brain Disease. I appreciated the clarity of its arguments.
The article opens with the following paragraph:
As an international network of historians and social scientists who study approaches to the management of drugs across time and place, we have noticed the effort to redefine addiction as a chronic, relapsing brain disease (CRBD). The CRBD model is promoted as a route to destigmatize addiction and to empower individuals to access treatment that works within that model’s terms.1 CRBD usefully recognizes that brain-based neural adaptations place individual brains in chronic states of readiness to relapse. But brains are housed inside of people. Substance use is biological, social, and political; our concepts and approaches to complex questions surrounding substance use must be, too.2,3 By overlooking the sociopolitical dynamics and inequalities bound up with substance use, the CRBD model can paradoxically further marginalize people who use drugs by positing them as neurobiologically incapable of agency or choice. We are concerned that the CRBD model paints drug users as individuals whose exclusion from social, economic, and political participation is justified by their biological flaws and damaged brains.
Note that the authors respond to an argument for what the disease model can accomplish — it “is promoted as a route to destigmatize addiction and to empower individuals to access treatment” — rather than to the argument that it is properly classified as a disease.
All illnesses occur within people and have biological, social, and political contexts. The past couple of years have reinforced that those contexts have important implications, even with something as seemingly straightforward as a respiratory illness caused by a virus. That COVID is associated with social, economic, and political disruption, conflict, and suffering shouldn’t and wouldn’t lead us to questions about whether COVID is properly framed as a disease.
Choosing between the CRBD model and addressing the sociopolitical dynamics and inequalities seems like a false choice. Why does it have to be either/or? Cant it, shouldn’t it, be both/and?
No responsible advocate of the chronic relapsing brain disease (CRBD) model would argue that people with addiction are incapable of agency or choice. Addiction is a disorder involving choice, but it is typically characterized as impaired choice or intermittent loss of choice, rather than a complete or consistent loss of choice. One might compare this to serious mental illness with intermittent fluctuations in impairment. These fluctuations in impairment may range from no impairment to severe impairment, depending on the individual and the current state of their illness.
It’s also important to note the authors’ switch from discussing the CRBD model in the context of people with addiction to people who use substances. The CRBD model should never be applied to people without addiction.
The article proceeds with a brief examination and critique of the CRBD model. The authors note that advocates of the CRBD model voiced hope that the model would produce a sharp break from the moral models that had dominated responses to addiction.
The supposedly new CRBD model recycles disease concepts that have mixed medical and moral concerns since the 18th century.9 Disease models have been used to support a range of policy approaches from strict prohibition, to compulsory treatment or “civil commitment,” to medical maintenance, to incarceration. In them, addiction has been both criminalized and medicalized; addicts were labeled as sick individuals yet also punished for bad behavior as deviants….
Despite the hopes placed on the new CRBD model, this heritage has not been erased by redefining addiction as a chronic disease located in the brain.11 On the contrary, the brutal social inequalities of US responses to drug-related harms have persisted or even worsened.
Note that this is not actually criticism of the CRBD. Rather, it’s criticism of the fact that the CRBD has not delivered the change in policy and attitudes that many people hoped for.
Framing Addiction as a Chronic, Relapsing Brain Disease
The article continues with the suggestion that the CRBD may have accelerated these harms in ways that include criminalization, incarceration, and a molecular orientation that opened the door for the opioid crisis with the false belief that Oxycontin’s extended-release formulation might make it safer.
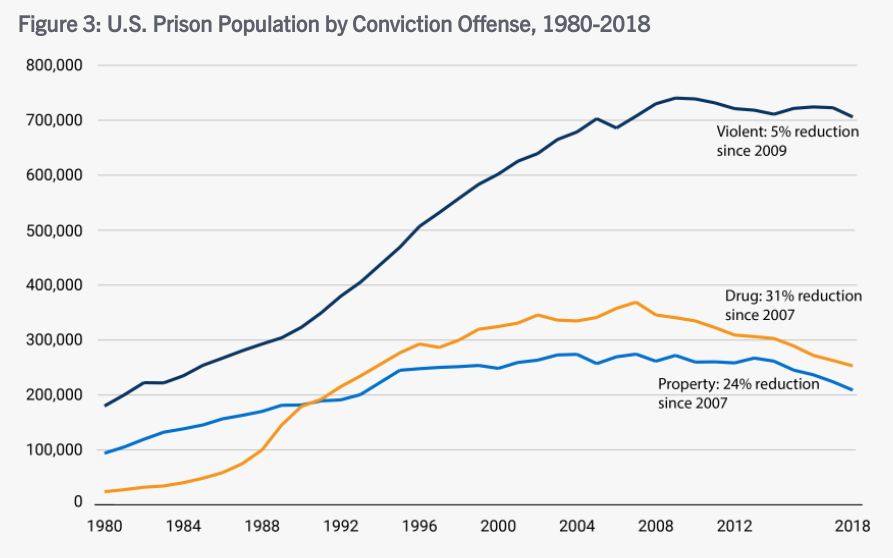
I’m not a believer that the CRBD necessarily leads to less stigma and better policy, and I won’t suggest that the CRBD is responsible for any changes in policy. However, the argument that the CRBD model is associated with incarceration is undermined by trends in incarceration for drug crimes. Even if the CRBD model could deliver significant policy and cultural change, that would take time — years, probably many years. The chart below shows a leveling off and eventual decline of people incarcerated for drug crimes during the period discussed. It’s still too many people incarcerated and those people are disproportionately African American but, if we want to assert an association between the CRBD and incarceration rates, the association would be a downward trend in drug crime incarcerations.
-

A liver cure containing 90% alcohol. -
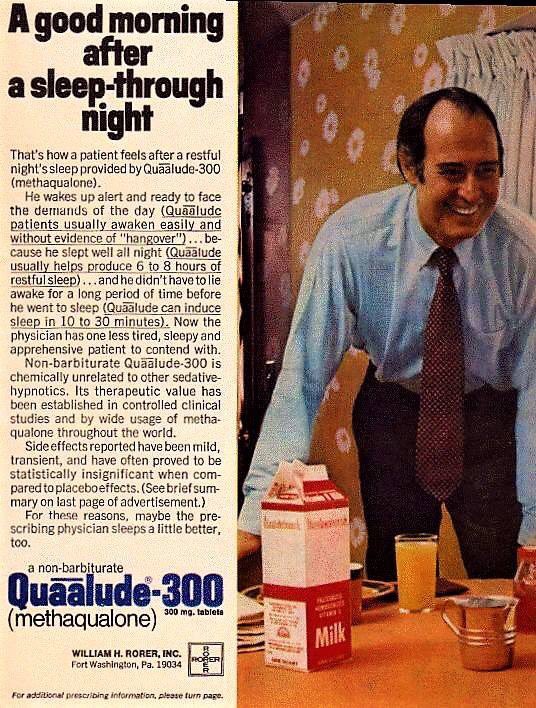
“mild… statistically insignificant side effects”
The Oxycontin argument would be a lot stronger if there wasn’t a long history of pharmaceutical advertising that misrepresented the safety profile of medications, often misrepresenting science to obscure the risks.
So… the criticism is not about the scientific or medical truth of the model, rather it’s about insufficient political and social progress.
This section ends with a strong point:
Expanding access to addiction medications without inclusive social policies and harm reduction has not been enough to prevent or stem America’s opioid crisis.
Calling something a brain disease does not and should not narrow our attention to pills and procedures. Behavioral, psychological, and social interventions ought to be particularly important with a brain disease, particularly since a brain disease is likely to affect those domains and those domains are largely experienced in the brain.
Alternate Frame: Harm Reduction and Social Justice
The authors offer harm reduction and social justice as an alternative frame:
There are other ways of framing and responding to substance use. The most promising of these is harm reduction, a 50-year-old social movement mounted against repressive drug policies. Rather than centering on the brain and embracing abstinence as a goal, harm reduction prioritizes the health and social inclusion of people who use drugs.
Note that the authors are not really speaking to causes or treatments and there’s no reason the recognition of a condition as a disease should omit social inclusion. For example, serious mental illnesses are recognized as diseases and social inclusion should be considered an essential element of effective treatment and policy.
So, what is the concern?
Consumers resist the coercive and often punitive ways in which medications for addiction have been deployed. Harm reduction links the biological to the social without prioritizing one over the other.
So, a concern is coercion. Calling something a brain disease does not necessitate coercion (think Parkinson’s), but it can open the door. In the medical world, that door might be opened through the legal designation of a guardian. With mental illness, involuntary treatment may be sought for patients that pose a risk to themselves or others. In the cases of guardianship and court-ordered treatment for a mental health crisis, there are processes designed to protect the rights of the individual, including time limitations on any court order resulting from the process.
In the case of addiction, involvement with the criminal justice system often leads to coerced treatment. And, there has been far too little systemic ambivalence about individual rights when it comes to coerced treatment (and incarceration) for addiction. Importantly, there’s also been too little concern about systemic injustices, like the disproportionate numbers of African Americans charged and convicted of drug crimes.
Addiction is also unusual among diseases in an important way. As Keith Humphreys pointed out, “To use a term from economics, addictions have high negative externalities that most medical disorders simply do not, and that changes how perfectly decent and reasonable people respond to them.”
To illuminate those high negative externalities, Humphreys poses the following questions:
If you had a financial manager who would have access to all your accounts and personal information, would you consider that person developing a heroin addiction of any more consequence than him/her developing type 2 diabetes? If you were enrolling your child in a preschool, would you react in the same way if informed that the teacher was prone to methamphetamine binges as you would to learning that the teacher was prone to asthma attacks? If asked by a non-expert from outside our field, how would you explain why millions of people have chosen to attend self-help groups and treatment programs focused on recovering from having had an ‘‘alcoholic’’ parent, but there is no demand for recovery programs focused on adult children of hypertensive patients?
Acknowledging that there has been insufficient concern for individual rights, I suppose at least 4 considerations are important regarding coerced treatment.
- Do the circumstances merit limiting the liberties of the person (through court supervision, incarceration, or coerced treatment)? Is this a circumstance where others were harmed or at serious risk of harm? If we removed the substance from the situation, would this still be a matter for the criminal justice (or child protection) system?
- Treatment for what? What is the person’s substance use problem and is the treatment appropriate for that problem? Are we talking about someone with a mild, moderate, or severe problem? Are we talking about someone with a pattern of impaired control?
- Coerced treatment is often an alternative to incarceration. This is a good thing. However, we should be mindful that this option doesn’t lower the bar for limiting the rights of a person.
- What systemic factors are likely to influence who ends up in this system and how their case is handled? Are we acknowledging and addressing those? If forces external to this system are a problem, how can that be mitigated within this system?
I’m ambivalent about the development of processes for addiction that would mirror the mental health processes. Having worked in both systems, I know it would require a lot of work to protect the rights of people with addiction and an enormous amount of work to develop systems of care that can meet the need effectively.
As for the role of the CRBD model in this area, I do see the risk and I do sometimes hear the CRBD model deployed to defend coerced treatment. At the same time, the period of time the authors point to has been characterized by efforts to reduce incarceration and offer treatment as an alternative — on the grounds that addiction is an illness.
I think the CRBD model offers a valuable test for public policy — parity. Would we, should we, treat a cardiac or diabetes patient this way? The high negative externalities identified by Humpreys do present a challenge for parity tests using other chronic diseases, but he offers another frame. He’s talking about it in the context of public education, but it’s relevant for thinking about policy as well.
A better analogy than asthma, type II diabetes, and hypertension we could employ for addiction might be to liken it to chronic infectious illnesses (eg, HIV/AIDS). We accept that for infectious illnesses, some fear of people who have the disease is rational; indeed health professionals exhort people to engage in behavior designed to protect themselves from infected individuals (eg, insisting that a sexual partner with a sexually transmitted disease wear a condom, not personally cleaning the body of someone who died from Ebola). Further, we accept that there is a legitimate role for law enforcement— Typhoid Mary was prevented from continuing to infect people by police (Marinelli et al., 2013), not doctors. Analogizing addictions to infectious diseases has all the virtues of analogizing it to diseases with low externalities (eg, asthma) and also has the unique advantage of better matching the public’s experience of the disorder (and it is them and not ourselves whom we need to persuade).
Of course, this imagery will evoke strong negative reactions from many, but it also provides the potential to narrow the focus for coercive interventions to those where there is actual harm or serious risk to others.
Uneven Progress: Harm Reduction in Europe
Next, the authors provide a little background on harm reduction in Europe that they summarize as follows:
Harm reduction initiatives across Europe and the United Kingdom were introduced as part of publicly funded institutions that often coexist with repressive drug policy systems—something shown with unusual starkness in the French example. The UK example indicates how harm reduction measures do not always center on social justice for people who use drugs but are instead introduced to protect the majority population. The Norwegian example points toward how restrictive access to harm reduction services can facilitate paternalism and reduce agency of people who use drugs.
Conclusion: Human Rights as an Expanded Harm Reduction Frame
…The human rights frame counters some of the CRBD model’s limitations, including the centering on brain disease pathology and insistence on judging each individual as either a patient or a criminal.
People who use drugs are themselves developing community-based harm reduction approaches that resist both criminalization and medicalization on the ground that both have been used to control drug users. Harm reduction critiques hierarchical forms of clinical and neuroscientific expertise and instead supports people who use drugs in recognizing their expertise in managing their own practices and bodies, supporting their agency, and widening their options. Abstinence can be considered part of this approach, but only if chosen by people who use drugs themselves.31 When abstinence is imposed by external forces (medical practitioners, family, law enforcement, or other stakeholders), abstinence itself becomes a risk for overdose death.
This illuminates another objection, that the disease label situates the person with addiction as a patient. (As opposed to a criminal.) It’s also important to note that the authors switched from addiction to “people who use drugs.” This switch is important because using drugs isn’t a disease but may be a symptom of the disease of addiction, just as coughing isn’t tuberculosis. To be sure, most people who use drugs do not have the disease of addiction. Differentiating between people with addiction and other people who use drugs is critically important in many ways, but particularly important when discussing the disease model, its conceptual boundaries, and its utility.
The framework of disease is helpful because it helps us draw a boundary to determine who has the disease and who does not, it can help us understand some of the processes involved and their consequences, it can help us identify treatments, and help us identify treatments, behaviors, and interventions that are contraindicated.
The authors seem to be very focused on protecting the right to choose to use drugs. For the minority of users with addiction, a critical element to understand is impaired control, meaning that drug use is not always freely chosen. (One might even say that, at times, the illness coerces the sufferer to use drugs. This is part of what’s so excruciating for people with addiction and their loved ones.) This is one of the reasons that, for this most severe form of drug problems affecting a minority of users, abstinence is indicated.
People with bipolar or schizophrenia have the right to refuse treatment in most circumstances. However, when their illness results in high negative externalities, they may be coerced into treatment via a process that includes several safeguards to protect their liberties.
So… this critique never seems to make a case that addiction is not a disease. Rather, it argues that the CRBD model has not delivered the change some people promised and they proposed a model centered on the social and political change. I don’t see where an emphasis on social justice requires the abandonment of the disease model. In fact, where high negative externalities are present, the disease model becomes a mitigating consideration, resulting in more just social responses.
I believe it’s true that addiction is a disease and the authors never really made an argument that it isn’t. Should that truth be sacrificed or obscured in pursuit of justice? I don’t think it’s a good idea. It’s the kind of thing that contributes to the current epistemic crisis and it isn’t necessary. Any model can be harmful if it’s misused or implemented in a reductive way that results in the neglect of important considerations. The CRBD is no different.
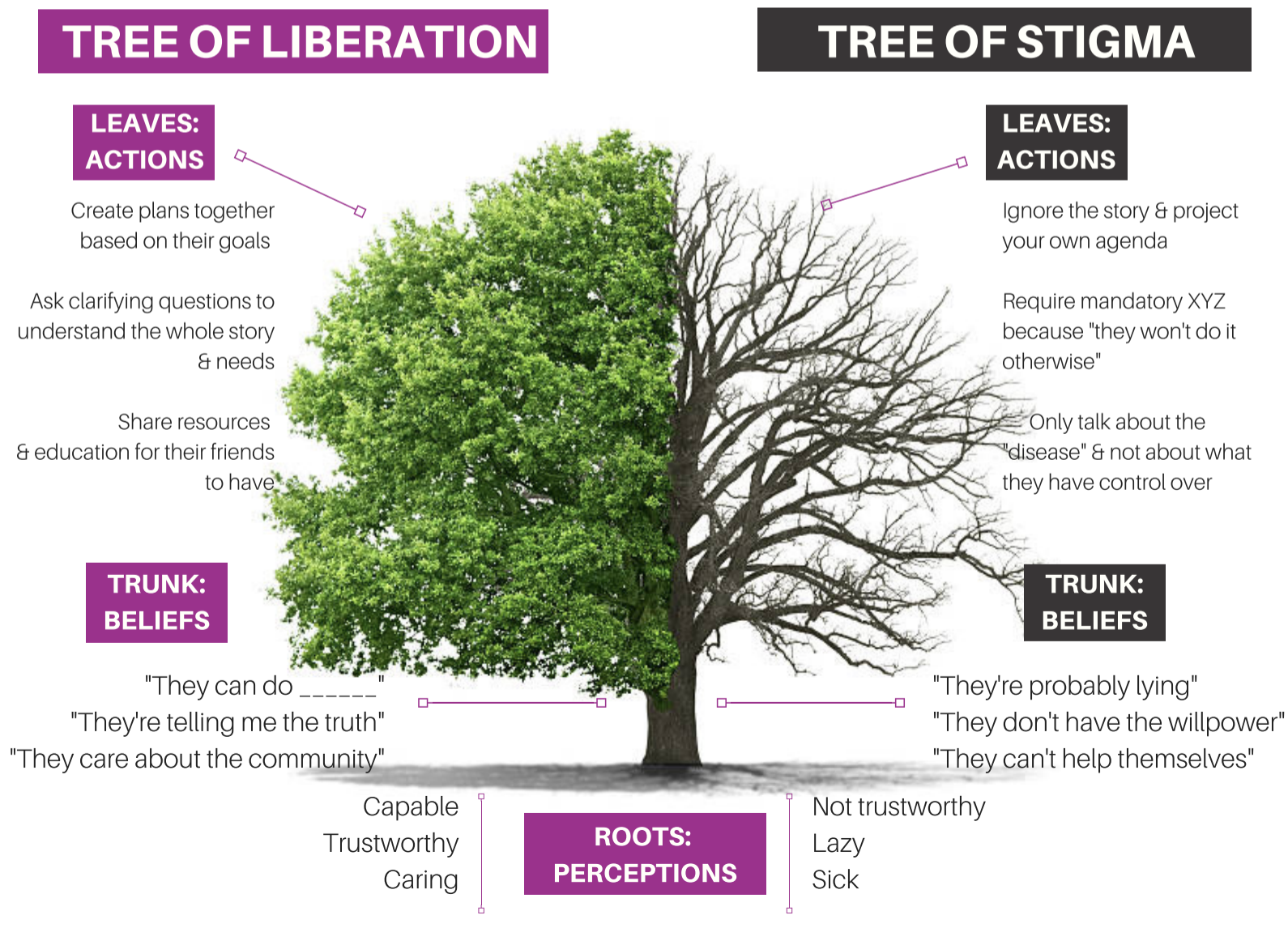
I recently stumbled on this educational page about stigma from the National Harm Reduction Coalition.
It’s well done and illuminates the assumptions and goals for their stigma reduction efforts. They frame responding to drug use as a choice between liberation and stigma, with harm reduction as the path to liberation.
While it may work for many (maybe most) people who use drugs, I’m concerned that it doesn’t work well for people with addiction and might require some modification if it’s intended to be helpful to this minority of people who use drugs.
They define stigma as follows:
Stigma is a social process linked to power and control, which leads to creating stereotypes and assigning labels to those that are considered to deviate from the norm or to behave “badly.” Stigma creates the social conditions that make people who use drugs believe they are not deserving of being treated with dignity and respect, perpetuating feelings of fear and isolation.
I’d emphasize isolation from their definition. To me, that is the essence of stigmatization. I see it as an evolutionary reaction to perceived threats, seeking to isolate the perceived threat from the rest of the community. That threat could be a disease, a behavior, or anything that might appear to be a threat to the health, function, structure, status, or social order of the community. (It’s important to recognize that something doesn’t need to be an actual threat and that evolution would favor the over-identification of threats. Further, many false positives will probably be aligned with the prevailing social structures, and ones that are not will often have post-hoc explanations that are aligned with those structures.)
In their framework, the goal for people who use drugs is liberation, which is described as such:
Liberation is the act of setting someone free from imprisonment, slavery or oppression.
In the context of drug use and sex work, liberation is about freedom from thoughts or behavior — ”the way it’s supposed to be” — and how we are conditioned to perpetuate harms to others.
The first statement emphasizes freedom — freedom from external forces infringing on liberty and dignity. The second statement adds freedom from harmful traditions and orthodoxies.
This strikes me as a place where it’s important to distinguish between people with addiction and other people who use drugs.
The elements above may provide a pathway to liberation from social responses to a freely chosen behavior. And, for most people who use drugs, it is freely chosen behavior.
The illness of addiction, however, is characterized by impaired control over use. Further, the experience of impaired control over drug use is an experience of oppression. This illness and impaired control constitutes a barrier to a life organized around the person’s goals, values, and priorities. These barriers extend into all areas of life — the relational, occupational, emotional, moral, civic, and spiritual selves.
Where the illness of addiction is present, freedom from external oppression cannot deliver liberation, though it may remove some barriers to liberation and recovery.
So, how might this change the tree of stigma?
My previous posts on recovery-oriented harm reduction shed some light on my ideas. However, reviewing the tree of stigma got me thinking that, while I differentiated drug use in addiction from other drug use, I didn’t speak explicitly enough to drug use by people without addiction.
Most drug use is not addiction. There is a broad spectrum of alcohol and other drug use. Addiction is at the extreme of the problematic end of that spectrum. We should not presume that the principles that apply to the problem of addiction are applicable to other AOD use.
ROHR is committed to improving the wellbeing of all people who use drugs. ROHR services are not contingent on current AOD use, recovery status, motivation, or goals. Further, their dignity, respect, and concern for their rights are not contingent on any of these factors.
Addiction is an illness. The defining characteristic of the disease of addiction is impaired control related to their substance use. We should not presume that the principles that apply to other people who use drugs will be applicable to people with addiction.
Drug use in addiction is not freely chosen. Because the disease of addiction affects the ability to choose, drug use by people with addiction should not be viewed as a lifestyle choice or manifestation of free will to be protected. It is not a expression of personal liberty, it is a symptom of an illness and indicates compromised personal agency.
An emphasis on client choice—no coercion. While addiction indicates an impaired ability to make choices about AOD use, service providers should not engage in coercive tactics to engage clients in services. Service engagement should be voluntary. Where other systems (legal, professional, child protection, etc.) use coercive pressure, service providers should be cautious that they do not participate in the disenfranchisement or stigmatization of people with addiction. Some might wonder whether ROHR is appropriate for people who use drugs and recovery is not an appropriate endpoint. (Because it isn’t indicated and/or wanted.) Its goal is to assure that hope and a visible pathway to full and stable recovery is available to all for whom it is indicated, but never to impose it.
For those with addiction, full recovery is the ideal outcome. People with addiction, the systems that work with them, and the people around them often begin to lower expectations for recovery. In some cases, this professional despair emerges in the context of inadequate resources. In others, it stems from working in systems that never offer an opportunity to witness recovery. Whatever the reason, maintaining a vision of full recovery (complete and enduring cessation of all AOD-related problems and the movement toward global health) as the ideal outcome is critical. Just as we would for any other treatable chronic illness.
The concept of recovery can be inclusive — it can include partial, serial, etc. While my ROHR writing has argued for a distinction between recovery and harm reduction, Bill White has described paths that can be considered precursors (precovery) to full recovery.
Recovery is possible for any person with addiction. ROHR refuses cultural, institutional, or professional pressures to treat any sub-population as incapable of recovery. ROHR recognizes the humbling experiential wisdom that many recovering people once had an abysmal clinical prognosis.
All services for people with addiction should communicate hope for recovery. ROHR recognizes that hope-based interventions are essential for enhancing motivation to recover and for developing community-based recovery capital. Practitioners can maintain a nonjudgmental and warm approach with active AOD use while also conveying hope for recovery. All ROHR services should inventory the signals they send to individuals and the community. As Scott Kellogg says, “at some point, you need to help build a life after you’ve saved one.”
Incremental and radical change should be supported and affirmed. As the concepts of gradualism and precovery indicate, recovery often begins with small incremental steps. These steps should not be dismissed or judged as inadequate. They should be supported and celebrated as personal accomplishments and they should not be treated as a clinical endpoint. Likewise, radical change should not be dismissed as unrealistic or unsustainable pathology.
ROHR looks beyond the individual and public health when attempting to reduce harm. ROHR wrestles with whether public health is being protected at the expense of people with addiction, whether harm is being sustained to families and communities, and whether an intervention has implications for recovery landscapes. It recognizes that the interests of people with addiction and other people who use drugs will diverge in many cases. ROHR maintains deliberate awareness of this reality and refuses to sacrifice one group for the other.
ROHR should aggressively address counter-transference. ROHR recognizes a history of providers imposing their own recovery path on clients while others enjoy vicarious nonconformity or transgression through clients. Substance use workers of all orientations are vulnerable to savior and martyr complexes. These tendencies should be openly discussed and addressed during training and ongoing supervision.
ROHR refuses to allow recovery and HR to be framed as counterforces to each other. While recognizing that most people who use drugs do not need or want recovery, for those with addiction, ROHR seeks to be a bridge to recovery and lower thresholds to recovery and avoids positioning itself as a counterforce to recovery. Recognizing that addiction/recovery has become a front in culture wars, ROHR seeks to address barriers while also being sensitive to the barriers that can be created in this context. When ROHR seeks to question the status quo, it is especially wary of attempts to differentiate from recovery that deploy strawmen, recognizing that this rhetoric is harmful to recovering communities and, therefore, to their clients’ chances of achieving stable recovery.
ROHR recognizes harm reduction can be an appropriate end for many people who use drugs, but is better pursued as a means to an end for people with addiction. ROHR views harm reduction as strategies, interventions, and ideas to reduce harm. As such, it is wary of models that frame harm reduction as an end unto itself for people with addiction. Back to Scott Kellogg’s point, “at some point, you need to help build a life after you’ve saved one.” The end we seek is recovery, or restoration, or flourishing, whatever is most appropriate for the individual or group. ROHR maintains awareness of tendencies to view harm reduction as “the thing” rather than “the thing that gets us to the thing.”
None of this is intended to suggest that anything here is bad or wrong. In the absence of addiction, this model makes a lot of sense. For most people who use drugs, it makes a lot of sense.
Historically, we failed to do a good job distinguishing between addiction and other drug use, erring on the side of categorizing far too much drug use as addictive. Appropriately, people have sought to correct this problem via professional, academic, and cultural change. (I’ve previously shared concerns about the DSM 5’s effect on the differentiation of addiction from other drug problems.) Unfortunately, this correction has resulted in the erasure of the distinction in many spaces.
This has been a good thing for people who had previously been miscategorized. They are more likely to be left alone and, where appropriate, get help that doesn’t presume addiction is the problem.
However, I’m increasingly concerned about the needs of people with addiction having their needs understood, respected, and responded to appropriately.
As the spectrum of drug use is increasingly being professionally, academically, and culturally understood as a manifestation of liberty and free choice, people with impaired control are likely to be misunderstood and stigmatized.
There’s no inherent incompatibility, but there is some tension. The needs and interests of people without addiction who use drugs, people with addiction who use drugs, people in recovery from addiction, the loved ones of those three groups, and the communities/communities of those three groups are not always aligned.
Recognizing these misaligned needs/interests is essential to developing models, systems, and policies that consider and respond to the needs of everyone. This would be important if these were stable and discrete categories, but the need seems even more important when we consider that people may move through these categories and may be in more than one category at the same time.
I recently read this article envisioning minimally disruptive treatment for opioid use disorder.
People who use drugs have long called for reforms to make opioid use disorder (OUD) care more patient-centered and less disruptive. Their calls align with broader healthcare transformation efforts, particularly to create “minimally disruptive” systems. Minimally disruptive medicine (MDM) is a “patient-centered and context-sensitive approach” focused on supporting patients’ life goals and health “while imposing the smallest possible treatment burden on patients’ lives.
My first reaction was to reflect on the reality that, over the years, most of my clients needed very significant disruption in their lives to achieve recovery — disruption in their social networks, cognitive models, emotional regulation, sleep, diet, family relationships, etc. Most of that necessary disruption occurred in the context of contact with addiction professionals and other people seeking recovery in treatment and mutual aid settings. That disruption is an essential part of the journey to becoming “better than well.”
I have that reaction as someone who has been a leader in efforts to implement a low-threshold prescribing model in an emergency department. However, I see that low-threshold practices as something akin to first aid and emergency care, rather than an effective treatment for a chronic illness. My wish is that those interventions prevent death, temporarily stabilize patients, and serve as an opportunity to engage the patient in a more comprehensive model of care.
I also recently came across the campaign Program, not a pill. The campaign appears to be a response to growing pressure in recent years to frame medication as an effective treatment on its own.
The majority of people with OUD have more than just OUD, and the medications don’t work for those other issues—common co-occurring conditions include other substance use disorders, mental health problems, difficulty functioning or working in society, social problems, etc. Comprehensive treatment programs can individualize care for each patient based on their own strengths, weaknesses, conditions and circumstances.
Not all 11 symptoms of OUD always respond well to medication treatment, so multiple interventions are necessary for the patient to stop use. That is, even if the physiologic symptoms are rather well addressed with medication, many patients continue to struggle.
Also, just this week, the Wall Street Journal has been reporting on the shortcomings of multiple digital behavioral health providers. Many of these services started with a vision of minimally disruptive care. Their reporting raises questions about whose needs are met with that model — the patient, or the treatment program?
These reactions, in no way, invalidate the Englander article’s critique of maximally disruptive practices. There’s no question that some disruptive practices are rooted in or propped up by stigma. The pandemic has provided a helpful opportunity to step back and examine some of those practices.
Yet, it also feels, to me, like we’re approaching an inflection point in the opioid crisis, where many families, policy-makers, patients, and providers are recognizing that we cannot prescribe our way out of the opioid crisis. This seems particularly important at this moment, as opioid settlement dollars flow into states and localities and, often, the easiest lift is to invest it in medications. (Despite the irony of returning restitution from pharmaceutical companies to pharmaceutical companies.)
So… where do all of these mental meanderings lead me? To be sure, some people will thrive with minimally disruptive models, but many will suffer and die without much more disruptive models. There’s a lot of variation in people’s pathways into addiction, their experience in addiction, and their pathway to recovery.
I suppose, rather than minimally disruptive or maximally disruptive, we ought to be focused on strategically disruptive models of care that do not rely on coercion and instead provide visible, realistic, and comprehensive pathways to recovery that will attract people voluntarily. It sounds easy, but this model was envisioned more than 20 years ago and, despite countless proclamations to the contrary, it’s never been realized at any large scale. It also runs against the zeitgeist (see here, here, and here), which frames patient-centered as organized around the patient’s short-term preferences that are often explored and understood in the context of systems and choices that offer no visible and realistic path to flourishing.

I’ve been hearing a lot lately about the difficulties in San Francisco related to severe SUDs among people experiencing homelessness. And more pointedly, I’ve been hearing about the death rate by overdose among those living in what I understand to be housing for these people provided by the city.
Simultaneously, I’ve heard reports about leaders in government (local, the state level, etc.) and in the SUD area at the national level, struggling with this puzzle in San Francisco.
Meanwhile, I’ve also had reports come across my view concerning significant financial allocations for broad use of contingency management to help people struggling in these ways, and to help cities improve their responses in these situations. And in that way improve the ecology of their cities.
A number of things come to mind for me in this context. One of them is the question, “What can San Francisco learn from Tehran?”
By that I mean, “What can leaders in the USA gain from partnering with those in other countries who have seemingly found locally relevant solutions, centered in people rather than professions, and are sustainable within existing local resources?”
An example of this kind of success is found in Iran and it’s called Congress 60.
For those not familiar with Congress 60 here are:
Sometimes it helps to learn from outside your discipline (a NIATx principle) and from an entirely different context (so we can see and hear and think in new ways).
The other thing that comes to mind for me is a set of lessons learned about contingency management.
During the lifespan of the Behavioral Health Recovery Management project (BHRM; 1998-2007 or so), we had a number of efforts including clinical dissemination of evidence based practices, best practices, and promising practices. These were per guidelines written for us by the first-author national experts in each area of improvement.
When we implemented contingency management in our outpatient methadone maintenance program (to help raise group attendance) we noticed that those pulling the “JUMBO” prize always returned the winning ticket to the fish bowl that held the tickets. We finally focused-grouped and asked “Why?” We were told very plainly that carrying the large screen TV down the street wasn’t safe.
In those years we partnered with other systems to build and run an FQHC (providing primary care, psychiatric care, SUD services, and access to public entitlements for housing and a whole range of those services). In doing so we were early innovators in embedding primary care and dentistry inside our OP psychiatric buildings. We found the show rate for a free dental cleaning was relatively high, and during that visit we could support with added psychiatric care down the hall.
The lesson learned was this: embed various kinds of services inside a location. People will come for what they want and need, and sometimes you can help by adding in less popular but equally critical assistance. That is to say, getting better initially in the way defined by the individual is contingency management (a relief and a reward). In that way you don’t define the “prize” and wellbeing begets other wellbeing.
In closing, here’s a link to a previous post about NA in Iran. That post includes a link to an audio upload that I find most inspiring. The upload comes to mind for me around the topic of culturally relevant local solutions that are sustainable and emerge from the community.
“I believe that the community – in the fullest sense: a place and all its creatures – is the smallest unit of health and that to speak of the health of an isolated individual is a contradiction in terms.” – Wendell Berry

We need to change how we think of recovery community organizations across our national care system. What is done is far too often managed by agencies not grounded in recovery community or narrowly funded in ways not inclusive of the diverse groups served. This kind of change would require us to explore uncomfortable truths and deep structural stigma within our institutions about addiction and recovery and embrace community as the true healing agent that it is.
We don’t collaborate with recovery community in ways that support its varied resources and strengths. To do so is perhaps the most important thing we could do to augment healing across our entire care system. As a corollary, we know that addiction counseling does not work well when it is overly prescriptive. Care must be individualized and engage the patient in ways that work for them for it to be effective. Why do we fail to apply this very same critical lesson to recovery community level engagement?
I started thinking about this after I ran across a post by Jason Schwartz – Sentences to Ponder. I then ran across the identical referenced section while reading Bill White’s retrospective – Recovery Rising:
“…I do want to suggest that something got lost along the road to professionalization. What got lost was a relationship between two people that transcended the roles of counselor and client. What got lost was our deep involvement in the community and in local communities of recovery. What got lost was our recognition of the power of community to heal and sustain people. John McKnight in his recent book, The Careless Society: Community and Its Counterfeits, argues that compassion shifted from a cultural value to a job description as paid helping roles replaced functions of families, extended families, neighbors, co-workers and friends. He argues that we don’t need more agencies or larger agencies, but that we desperately need more community. In medicalizing alcohol and other drug problems in hopes we could escape its social stigma and moral censure, we turned our backs on the power of community and created an ever-growing distance between ourselves and those we are pledged to serve.”
Bill was writing about Robert McKnight book, Careless Society: Community and its Counterfeits. We do great harm to the community we serve when we prescriptively dictate a narrow set of goals for them. We rob agency from the community and improperly shift power to the external agent. In a parallel process, one of the things that make addiction counseling so special is that when it is done properly, it holds space for healing in a spirit of humility and deep empathy. Bill White describes it well in a piece he did for Counselor Magazine in 2004 titled “the historical essence of addiction counseling.” It honors healing as a highly individualized process not under the rigid control of the counselor.
Honoring Individuals in Care by Holding Space to Explore Their Inherent Strengths and Resiliency
Seasoned clinicians know that we fail the people we serve when we are overbearing or too prescriptive in the therapeutic relationship. Reflecting on my early years as a counselor, I learned fairly quickly that my way was not the best way or even the right way.
Like many new counselors, I made a lot of mistakes. I thought I knew what the person needed to do and could essentially dictate their care. My false expectation was that I would tell them, they would listen, and change would occur. Thankfully, I learned quickly and overcame my misguided thinking. I learned change is a highly individualized process. People must be involved and steer their own recovery process for it to work over the long term.
In those early days, I lacked insight into the full spectrum of strengths the people I was working with possessed. Most of our forms in our service systems focus on deficits when what we should emphasizing is their strengths and the ecology of the communities they live in. People are so very much more than the labels and deficits endlessly delineated in the paperwork we all gathered every time they drew the courage to walk through our doors.
My effectiveness dramatically improved as I learned more of the craft of being a good counselor. I listened more deeply and reflectively. I helped people explore who they were, why they reacted as they did and most importantly the incredible resources they had, but far too often had hidden from themselves. This kind of change takes time and open examination. I was gifted with good mentors and a care system that did not jam people through the process too quickly and fail them in the long run.
I learned so much from the people I was privileged to work with. I learned people are resourceful and resilient. I learned that people who walked into my offices in rags and carrying all their possession on this earth in a trash bag were capable of dramatic change beyond either of our most optimistic initial expectations. I learned that every individual has resources we miss unless we hold safe space for them. A place to explore and nurture the immense capacity for positive change every human possesses. A process that heals people in ways I could never predict or control.
It healed me too. It helped keep me stay vital despite what was occurring around me. The work of helping people within our public care systems is profoundly difficult. I have witnessed a lot of pain and destruction. I have seen and experienced a great deal of trauma. Our systems, insensitively burying us in paperwork, even as we tried to wade through it to help people heal in ever shorter durations of care at lower levels of intensity than what the person needed to get better. I am glad my formative years occurred before services became so constricted.
There is a dark side of our care systems just like every other institution, yet through it all, I, like many other veteran workers who stayed with the work saw that we could, at times be part of a miracle. I have spoken to a lot of service providers and every one of them to a person identified this is why they stayed doing the work, to be small part of the transformative process. To help nurture healing which emerges as hope, purpose and connections are restored.
Honoring Recovery Community as Force of Transformative Healing with Inherent Strengths and Resiliency
I took on a project a few years ago to understand how the New Recovery Advocacy Movement came to be. There would have not been a movement that transformed the way that America understands and talks about recovery without the SAMHSA Recovery Community Support Program (RCSP) grants. Having conducted a number of key interviews with the original grant recipients, the federal grant officer was identified by several interviewees as key to what was accomplished. I interviewed Cathy Nugent to try and find out what it was that she did that helped them come together.
I learned she was a clinician skilled in the art of group process. She brought the grant holders together and helped them see their own strengths. She acknowledged that she was not an expert on recovery, that people in recovery are the real experts. She used her skill set to help those initial RCSP grant holders to develop their inherent strengths.
I once heard Don Coyhis, founder of White Bison, and a key leader in the Wellbriety movement talk about that grant. He shared from a podium about being asked to conduct it using evidence-based practices, He noted that the Native American community had several thousand years of what worked for them and asked how many years of evidence the federal government had.
In an act of wisdom the strengths of this community were respected. They were not diminished by the bureaucracy. Honoring the strengths of that community was the proper action and illustrative of what our system must do more broadly. Communities are diverse. Each has its own culture. They can blossom when provided the proper resources. A sum far greater than its individual parts.
How we fail people in care and communities of recovery when we do not hold space for them:
- We rob them of their own autonomy and stifle their inherent creativity.
- We fail to honor their inherent strengths by restricting them to our limited vision of what they can accomplish.
- We limit their capacity to actualize and help their own members heal in ways that they know far better than we do.
- We impoverish our entire system from a deeper reservoir of resources, skills and social connections to draw from.
What would recovery look like if we supported recovery in communities in ways that honored community diversity and strengths? I imagine what would happen is similar to what happened when I shifted my individual practice, and I was more open to possibility. The people I served went farther than I could imagine when I got out of their way.
What a lesson. What possibility.
We have not done nearly enough to unleash the power of change waiting to emerge from within our recovery communities across America. We stand on the verge of nearly infinite possibility. To deeply honor and support the healing power of community would be to shift our paradigm of healing to the exact thing our nation needs more than anything else at this point in history. More cohesive community.
I dare to imagine we can accomplish so much more than we are now.
I hope you do too.

Yesterday’s post about efforts to support recovery in San Francisco brought some of Bill White’s blog posts and this video from the HBO Addiction series to mind. (The video is showing its age with respect to some of the language and content, but it conveys some very salient lessons that haven’t changed.)
From Bill White:
Physical places and sociocultural contexts exert profound effects on human behavior–a reality too often ignored within biological models of addiction. The repertoire of behaviors that constitutes the states of addiction and addiction recovery are far more than an expression of intrapersonal vulnerabilities and strengths–more than a mirrored expression of genes, character, and personality. Personal behavior can reflect the influence of or domination by the ecosystems in which one is nested/trapped. This suggests the need to extend our focus beyond the intrapersonal to the ecology of recovery–creating social contexts that elicit recovery and suppressing contextual factors that increase risk of addiction.
So, do we continue to send fragile recoveries into environments in which only the strongest recoveries survive? Or do we build recovery-friendly communities in which even the most fragile recoveries have a chance of survival? Those are the questions we face as a country and as people working in the addiction/recovery arenas. We must always attend to recovery at a personal level, but we must also think about recovery in its local, regional, national, and global contexts. Both addiction and recovery are a reflection of the ecologies in which they are nested.
This article from the San Francisco Chronicle caught my attention this week. It illustrates the challenges big cities are facing with the combination of the behavioral health crisis, the aftermath of the pandemic’s disruption, noncarceral responses to drugs, the lack of affordable housing, social responses that frame addiction as secondary to other problems, and the absence of systems of care that deliver addiction care of adequate quality, intensity, duration, and scope.

The article focuses on overdose deaths and the reality that, in recent years, more than 40% of OD deaths in the Tenderloin occurred in sites used to house homeless people, and more than 16% of the city’s OD deaths occurred in single room occupancy setting that are part of the city’s housing program.
“We take people off the streets and put them in this environment they’re not ready for — due to mental illness, or trauma or substance abuse — and sometimes they get worse,” he said.
Even if people like Jackie want to live in supportive housing units where drugs are not tolerated — a model sometimes referred to as recovery housing — there are no permanent, publicly funded options for them in San Francisco. Currently, a formerly homeless person seeking a sober living environment would need to enter a temporary rehabilitative program rather than long-term housing.
So… they don’t have recovery-safe housing and the alternative is treatment. What happens when they complete treatment? Where do they live then?
Cohen said that the agency has heard from some tenants who would “prefer to be in a sober environment and have more choices within” permanent supportive housing. But, Cohen said, HSH’s stance is that abstinence-based programs are “not an evidence-based best practice” and therefore the department has no plans to pursue the model.
This is just not true. There’s considerable evidence supporting recovery housing. It’s not just a few studies and it’s not a recent development.
Sober living environments raise difficult legal and ethical questions, according to some drug policy experts. Critics say residents may hide their drug use at the worst possible time: when their tolerance has worn off and they’re most at risk of overdosing. The model could create a revolving door back to the streets as tenants are kicked out for using.
These concerns represent real challenges to the model, but they are not unsolvable. Systems of care and providers ought to be held responsible for developing and using processes to maintain engagement, restabilize relapsed residents, adjust treatment plans accordingly, and provide a pathway to maintaining or re-entering housing. There also ought to be safety net services for residents who cannot be restabilized and re-engaged. When residents know these processes exist they are more likely to report their relapse or the relapse of a housemate and the addiction can be interrupted–preventing overdoses.
Residents and patients also ought to participate in meaningful informed consent at multiple intervals throughout their early treatment and recovery journey, and they ought to have easy access to the pathway of their choosing with continuous recovery support.
Still, a growing coalition of advocates, including San Francisco Supervisors Ahsha Safaí, Catherine Stefani and Matt Dorsey say the city should explore more types of housing programs that would allow people to live in a drug-free environment.
“We should do more to make sure that people who have substance use disorder have more options than just being in an SRO in the Tenderloin where drugs are surrounding them,” Stefani said in an interview. “It is ridiculous to think that anyone can recover in those circumstances.”
What I appreciate from these advocates is their refusal to turn policy responses into false choices between protecting the lives of people who are using drugs, people choosing treatment/recovery pathways involving agonist medications, and people choosing agonist-free pathways.
One of the other important things I detect in Dorsey’s San Francisco Recovers model is the way they view people with addiction.
Years ago, I was involved in the development of an SUD program for young people in the criminal justice system. A partner in the development of that program said that “we can view these kids as perpetrators, victims, or resources.” Of course, one doesn’t have to cancel out the others, but it was a good reminder to check our mental models and approach those kids as resources.
I sense that same spirit in this model. These aren’t perpetrators to incarcerate or isolate. They aren’t victims to pity, infantilize, and expect nothing from. They are resources that need some help at the moment.
UPDATE: A friend just commented that this is a reminder of how easily compassionate and well-intentioned responses to addiction can devolve into something that resembles an addiction hospice. And, when we construct addiction hospices, we shouldn’t be surprised that people die.
As SMART Recovery meeting facilitator Jeffry Muhleman sees it, the journey to a full-blown substance use disorder is never intentional. “The crazy thing is that when you take your first drink or first hit, nobody tries anything and says, wow, that’s so good I’m going to become addicted to that.”
For Jeffry, it began in 2008 at a New Year’s Eve party where he tried crystal meth for the first time. From there he tumbled down a twelve-year rabbit hole of substance use, bad choices, and legal trouble. Once he found SMART, his journey turned in a whole new direction.
Jeffry attended a variety of meetings and found that some resonated with his experiences more than others. Then he got to thinking, “Being an out gay man, I realized that there was really a need in the recovery community for meetings that are appropriate [for individuals who identify as LGBTQIA+].” Motivated by the value he found in SMART, he decided to become a facilitator and start a meeting specifically for members of the LGBTQIA+ community. But that didn’t mean he wanted to change the way SMART Recovery works.
Jeffry believes that SMART Recovery can work for anyone regardless of sexual orientation or gender identity. That said, he also supports the availability of population-specific meetings. “The reason SMART offers meetings for the LGBTQIA+ community (and other groups) is to provide a forum where common experience and unique understanding inform the conversation.”

Jeffry notes that humans are inherently familial and social, and sharing recovery with those who can closely identify with one’s experience is very beneficial. He also points to the value of therapies that increase a person’s self-awareness and mindfulness, along with the use of SMART tools.
It all comes together in a supportive way for individuals, no matter their perspective or experience. Jeffry says every SMART meeting he’s attended has been safe, and the sheer variety of meetings creates a successful recovery pathway that is available to all.
As seen in Jeffry’s story, when one person decides to help another by giving of their time and energy, it makes a large impact. Jeffry took what he learned from participating in support group meetings and started his own meeting serving the LGBTQIA+ community. His contribution has made it possible for SMART to reach more individuals who are asking for support.
Your year-end financial contribution will be put to work immediately to make additional efforts like this possible. Like Jeffry, you will help more individuals embrace Life Beyond Addiction.
Additional Resources
PLEASE NOTE BEFORE YOU COMMENT:
SMART Recovery welcomes comments on our blog posts—we enjoy hearing from you! In the interest of maintaining a respectful and safe community atmosphere, we ask that you adhere to the following guidelines when making or responding to others’ comments, regardless of your point of view. Thank you.
- Be kind in tone and intent.
- Be respectful in how you respond to opinions that are different than your own.
- Be brief and limit your comment to a maximum of 500 words.
- Be careful not to mention specific drug names.
- Be succinct in your descriptions, graphic details are not necessary.
- Be focused on the content of the blog post itself.
If you are interested in addiction recovery support, we encourage you to visit the SMART Recovery website.
IMPORTANT NOTE:
If you or someone you love is in great distress and considering self-harm, please call 911 for immediate help, or reach out to 988 Suicide & Crisis Lifeline @ 988, https://988lifeline.org/
We look forward to you joining the conversation!
*SMART Recovery reserves the right to not publish comments we consider outside our guidelines.*
Brian Coon posted a reaction to the NIAAA definition yesterday. I also recently watched the NIH webinar on the definition.
“Recovery is a process through which an individual pursues both remission from AUD and cessation from heavy drinking. Recovery can also be considered an outcome such that an individual may be considered ‘recovered’ if both remission from AUD and cessation from heavy drinking are achieved and maintained over time. For those experiencing alcohol-related functional impairment and other adverse consequences, recovery is often marked by the fulfillment of basic needs, enhancements in social support and spirituality, and improvements in physical and mental health, quality of life, and other dimensions of well-being. Continued improvement in these domains may, in turn, promote sustained recovery.”

I like several elements, including ones that Brian noted:
- It frames recovery as a process and an outcome. (Other recent definitions frame recovery only as a process.)
- It provides clear criteria.
- The criteria address alcohol use.
- It looks beyond drink counting and references improvements in global health and quality of life. (Note, though, that these improvements are not required.)
All that said, it leaves me wanting something different.
As I sat with that dissonance, I decided that it is a fine definition of recovery for Alcohol Use Disorder (AUD) but I find myself troubled by the application of the concept of “recovery” to AUD.
In the webinar, John Kelly discusses (15:30) the challenge of trying to turn a cultural concept (recovery) into a scientific concept. The cultural concept of recovery is more than the reduction (or even elimination) of symptoms and focuses on an additive experience. I think it’s also fair to say that, in the cultural realm, recovery has been more than a process or outcome–it’s been an identity.
Why would something recovering from an illness become integrated into one’s identity? Because the experience of alcohol and other drug addiction is often life-threatening, traumatic, treatment can provide few guarantees, and it often erodes one’s identity. It also transforms an experience of stigma into an identity the individual feels pride in.
So, when you’re talking about recovery as a kind of identity, “recovery from what?” becomes a salient question.
People who faced and survived a life-threatening illness like lung cancer may integrate being a cancer survivor into their identity. The same might be true for groups of people who survive certain disasters. Importantly, those identities may serve as a source of connection to others who share the identity and can be powerful enough as a social adhesive that entire communities are built around them.
This definition puts the following people into the same category of “recovery” from AUD:
- While in college, Henry drank several days a week, spending most of the weekend drinking with friends. During his sophomore year, it was common for him to have as many as 8 drinks on weekend days, but that progressed to 12 during his junior year to achieve the same effect. It was common for him to be hungover on Saturday and Sunday mornings and spend half the day recovering. His drinking caused considerable tension with his parents who believed his drinking adversely affected his grades and his relationships with his family. This was true, but Henry said he wasn’t concerned. After a few rough semesters, Henry decided to cut back to a couple of drinks on Thursdays and 4 drinks on Fridays, Saturdays, and Sundays.
- Shayna started drinking in her teens and drank heavily on weekends, often drinking to the point of passing out. On a couple of occasions, friends needed to take her to the hospital for alcohol poisoning. She tried to cut back, but found herself unable to moderate with any consistency. Shayna got into a good college, but her drinking led to her being expelled due to poor grades. Several relationships ended because of her excessive drinking and her behavior when she was intoxicated. She lost jobs due to her drinking and tried to stop but was unable to, despite her best efforts. Her parents took physical custody of her children because her drinking made her an unreliable caregiver. She entered treatment several times but dropped out or never stopped drinking despite anti-craving medication. She spent time in jail due to multiple impaired driving convictions. She entered treatment for the 8th time, moved into a recovery home for 12 months, got deeply involved in a mutual aid group, stopped going to old hangouts, and developed a new social network of people in abstinent recovery. She struggled with severe cravings to drink, fortunately, these faded slowly as she did the hard work of rebuilding her life.
- Mark had a pattern of alcohol use very much like Shayna’s but also used cocaine, cannabis, and opioids. After a drunk driving accident, Mark found that using benzos helped him reduce his drinking to a few drinks a few times a week. Others have noticed that his cocaine use accelerated following the reductions in his drinking. His drug use is causing considerable functional impairment and he meets all criteria for substance use disorder.
Does it make sense to put these three people in the same category? They’re all in remission from AUD and have ceased heavy drinking.
Would Henry or Mark be likely to identify as in recovery? Might they begin to use that label if researchers, treatment providers, and advocates tell them they are in recovery? Would their loved ones think of them as in recovery? Would it make sense to an observer if we describe them as being in similar states of recovery?
To me, remission seems like a more appropriate characterization of Henry’s experience.
On the other hand, it would seem strange to characterize Mark as in recovery from AUD when he is in the throes of drug addiction.
Would Mark, Henry, and Shayna see themselves as having a shared experience or identity? Would their experiences be helpful or validating to each other? How meaningful is a category that includes such diversity in pathology and problem resolution?
Putting the three of them in the same category may make sense from the perspective of a researcher (I’m not sure that’s true.), but does it make sense from a cultural perspective? Does it make sense to develop research definitions that create discord with cultural understandings (even if their boundaries are poorly defined)? Where there is discord, how do research and cultural understandings interact and influence each other?